

Gummadi Ashish1
Coresponding Author:
1Senior Physical therapist, Department of Neurorehabilitation, Institute of Neurosciences, Kolkata, Mail id: ashishgummadi@gmail.com
| Aim and background of the study: Pes Anserine Bursitis is an inflammatory condition of pes anserine bursa which affects medial and inferio- medial aspect of the knee with more painful and swelling around the knee joint. Aim of the study is to find the effectiveness of iontophoresis and open kinematic chain exercises on pain, and knee range of motion of sports person with pes anserine bursitis. Methodology: 30 male and female subjects according to inclusion and exclusion criteria were randomly divided into two groups for the study where, Experimental Group was treated with Iontophoresis and open kinematic chain exercise. Control Group was treated with Ultrasound therapy. Result: The study reported the Group treated with Iontophoresis and open kinematic chain exercise got significant improvement in VAS and KROM score with p=0.001. Conclusion: the study concluded that the experimental group which received iontophoresis along with open kinematic chain exercises demonstrated good effect in reducing pain and increasing Knee ROM. Key Words: Iontophoresis, open kinematic chain exercises, Pes anserine bursitis, VAS, KROM. |
| Received on 14th January 2021, Revised on 22th January 2021, Accepted on 18th February 2021; DOI:10.36678/IJMAES.2021.V07I01.001 |
INTRODUCTION
Knee is a hinge variety joint, which provides flexion and extension movements and a small degree of medial and lateral rotation. Pes anserine bursa of knee joint get inflamed due to over use and the bursitis affect medial and inferio- medial aspect of the knee with more painful and swelling around the knee joint 1, 2.
Pes Anserine Bursitis Epidemiology: Pes anserine bursitis is a common in running sports person. It is self-limiting condition, it can be cure with surgery or without surgery.1Pes anserine bursitis risk increases with endurance sports (distance running or triathletes), making changes to or beginning a new training program, sports that place stress on the muscles that insert at the pes anserine, such as those that require pivoting, cutting or, jumping, improper training, poor strength and flexibility, failure to warm-up properly before activity, improper knee alignment (knock knees), arthritis of the knees and trauma or constant friction on the bursa3.
Pes Anserine Bursitis in Sports Person (Marathon Runners): Pes Anserine bursitis risk is higher in endurance training and one of the most frequently affected individuals are Marathon Runners as they performs lots of endurance training. Usually in marathon runners, the tendon may become overused due to change in the training- for example running more uphill or just increasing the intensity of training program. Or any change in footwear can also be a cause 4.
The new runners or those who have not had a professional gait analysis can develop Pes Anserine Bursitis. This Bursitis may develop over the course of long run, or may be a few weeks. Whatever be the duration, the main cause is due to overuse of the tendons that guards the pes anserine bursa.6
Pain in the inner aspect of knee, swelling and difficulty to bend the knee are the main symptoms of Pes Anserine Bursitis. Later stage muscle around the knee which produce extension and flexion movements may go for week followed by reduce the range of movement in knee joint 5.
Physiotherapy is the most widely used form of treatment adopted for gaining relief from pes anserine bursitis. It is used in both modes as single line of treatment including exercises or in form of combination with electrotherapy modalities like Ultrasound, Iontophoresis etc. The exercises include stretching, strengthening, ROM exercises. In flat feet individuals suggests with wearing arch supports in their shoes. Compression bandages or knee sleeves also helpful for reduce symptoms 6,7.
Iontophoresis is a therapeutic technique in which ion transfer into the body tissues by using electrical current as a driving force (LeDue, 1903).Iontophoresis is painless, sterile and non-invasive method to introduce specific ions into the body tissues. In case the ions are used in the form of ointment, a layer of its applied at the site to be treated. Iontophoresis treatment with dexamethasone is well tolerated by the majority of the patients5.
Open kinematic chain exercises (OKC) are the form of exercises in which the distal segment is mobile or not fixed like isolated joint exercise e.g. Seated leg extension. Open kinematic chain exercises are helpful to correct strength deficits of specific muscles or joints and beginning of rehabilitation when athlete not able to perform CKC exercises.11Open kinematic chain exercises are helpful to gain strength, flexibility and endurance of.3 hamstrings muscles group in sports person affected with Pes anserine bursitis8.
To evaluate the pain intensity VAS has been used whereas Knee ROM was measured using Goniometer. This study aimed to find the effectiveness of both the intervention in sports person with Pes Anserine bursitis.
In this modern age, there is a need of active research on an easy and effective intervention to reduce the pain and gain the near full ROM which enhances the performance in sports person.
Many Pes anserine bursitis patients experience pain, muscle weakness, decreased ROM and functional disability. Most patients regain their ROM muscle strength within a few week, but between 30 to 50 % are no longer able to get full ROM, muscle strength and functional ability after 1-2 month. So there is a strong need to gain full ROM muscle strength and pain reduction in Pes anserine bursitis rehabilitation .The persisting problem of ROM at knee muscles weakness and increased pain needs to be addressed and newer strategies such as Iontophoresis with open kinematic chain exercises can bring better insights for sports person with Pes anserine bursitis7,8.
In this study, iontohoresis with dexamethasone sodium and open kinematic chain exercise has been used to treat the sports person diagnosed with Pes Anserine bursitis.Iontophoresis is a therapeutic technique in which ion transfer into the body tissues by using electrical current as a driving force (LeDue, 1903).
Iontophoresis is painless, sterile and noninvasive method to introduce specific ions into the body tissues. In case the ions are used in the form of ointment, a layer of its applied at the site to be treated.11Iontophoresis treatment with dexamethasone is well tolerated by the majority of the patients and is effective in reducing symptoms such as pain and tenderness and better enable patients to tolerate therapeutic exercises and, therefore, will accelerate the rehabilitative process8.Hence this study is an attempt to find out the effectiveness of Iontophoresis with Open kinematic chain exercises (OKC)
METHODOLOGY
The subjects for the study were taken from the outpatient department of Neuro-rehabilitation Instuite of neurosciences kolkata. The subjects referred to the physiotherapy department with the diagnosis of Pes Anserine bursitis were screened for inclusion and exclusion criteria. The subjects who were qualified for the trial will be explained the aim and objectives of the study.
The subjects were requested to sign the consent form. The subjects were measured for their baseline outcome measures. A total 30 subjects who fulfil the inclusion criteria were included for the study and allotted into 2 groups, Experimental group (EG) and Control group (CG) randomly. The subjects with both groups received intervention for 12 days, the baseline measurements will be compared to the data at the end 12 days.
Procedure of intervention for the experimental group
Iontophoresis: Dexa-methasone sodium phosphate 0.4% with aqueous water was given via Galvanic current. The current used for this process was kept 1mA with subjects comfort considerations. In Iontophoresis current density always depends on quantity of current delivered per unit surface area. For this, two electrodes are used negative electrode (cathode) and positive electrode (anode), Negative electrodes used was double the size of the positive electrode. Since Dexa-methasone sodium phosphate is negative ion (-), it was placed over the cathode (-). The cathode was placed over the pes anserine bursa where as the anode was placed over the calf muscle. Duration for iontophoresis was 20 minute per session once a day for 5-7 days 3
All the 15 patient of experimental group treated with Iontophoresis for initial 5 days were then treated with Open kinematic chain exercises (OKC) for knee everyday two session each session consisting of 30 minutes .Each exercises was performed with proper rest period of about 2 minutes after each exercises. Patient performed these exercises in supine lying position and support was provided by te assistant as necessary.
These exercises included the following exercises-
Hamstring stretch on wall: Subjects was in supine lying with hands by side, subjects involved leg on wall and other leg as free, as instructed by examiner, 10 repetitions were done with feel stretch.
Single leg hip extension: The patient was asked to lie down on his back with his knee bent at 90 degree and his feet hip width apart. From this position patient was asked to raise the leg and hold it suspended. Then the patient was asked to push his hips and lower back as one unit through the stabilizing leg, keeping his weight centered at his heel.10 repetitions with 10 counts hold
Seated knee extension: Subjects was in high sitting position, and the patient was asked to straight the knee.10 repetition with 10 count hold
Straight leg raise (SLR): The non-affected leg was flexed for 90 degree at the knee joint; the affected lower limb is straight on the table. The patient was asked to raise the affected lower limb straight to the level of the other leg.10 repetitions with 10 count hold.
Procedure of intervention for control group
Each participant in this group received ultrasound therapy with the intensity ranging from 0.8 -2 W/cm2 for 8 minutes in pulsed mode. The subject was positioned in high sitting position with the knee slightly rotated outward and the other leg of the subject was asked to keep apart from the involved limb. The ultrasound was given by the therapist over the painful area in small concentric circles.33
Method for outcome measures
Visual Analogue Scale (VAS): VAS was used to measure subjects perception level of pain due to Pes anserine bursitis .It consists of scale where scoring is from 0-10. With score 0 subjects express no pain and with score 10 expresses maximum pain. The patient was asked to level the highest amount of pain they were getting at the time of assessment.
Knee Range of Motion (ROM)-Goniometry: Knee ROM includes flexion and extension which was measured by goniometer. To measure knee flexion, patient was asked to lie down in supine position and the subject was asked to bend the knee. Three trials of the same procedure were performed and average of the readings was considered for data analysis. To measure Knee extension, the patient was asked to lie down in prone position. The subjects was instructed to lift the knee without pelvic tilt (stabilize femur) and then goniometer was placed and the average reading of the three trials was recorded.
Inclusion criteria: Subjects between ages of 15-30 yrs. Both genders were included. History of improper training, running up hills with trackers, which produce pain and tenderness localized near Pes anserine bursa, Marathon runners, running for > 2 years were selected for the study.
Exclusion Criteria: Subjects with stress fracture, subjects with other lower limb musculoskeletal pathology, subjects with ischemic disorder of lower limb, subjects with muscle spasm of hip extensors, malignancies or tissue damaged by radiation therapy, subjects with visual impairment or with any other neurological
disability like any head trauma, dementia, learning disorder and schizophrenia, and Osteoarthritis of knee were excluded from the study.
Materials and Methods: It includedCouch, EMS/Galvanic, Dexamethasone sodium phosphate aqueous solution, Cotton, Microspore tape, Goniometer, Ultrasound machine, and Aquous gel
Outcome Measures: Visual analogue scale (VAS) and Knee range of motion (ROM) goniometry
RESULT
Study design: A Comparative two group interventional clinical study
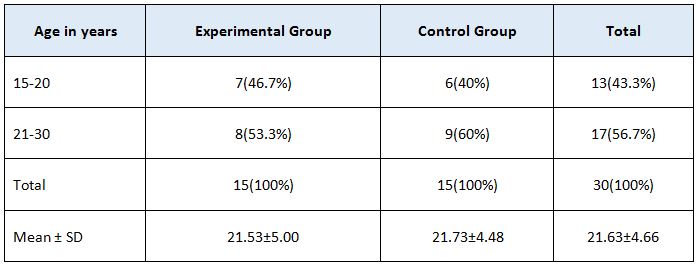
Table 1 show that there is 46.7% of patient in Experimental group and 40% in Control group of age group 15-20. However, 53.3% were in
experimental group and 60% in control group
of age group 21-30.
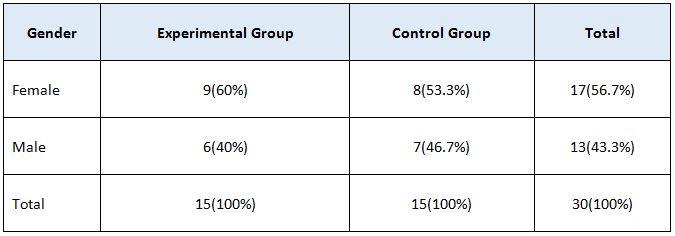
In table 2, Experimental group consists of 60% female and 40% male whereas control group consists of 53.3% female and 46.7% male patients. Overall, 56.7% of patient was females and 43.3 % was males.
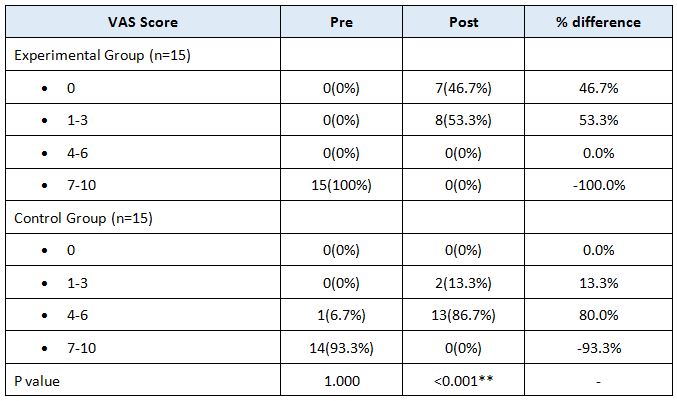
VAS score of both the group were analysed in table 3 and the mean difference in percentage was obtained. Range of VAS scale score was made as 0, 1-3, 4-6, 7-10 in both the groups. The VAS score has been significantly reduced in Experimental Group as compared to Control Group. In the VAS score the % difference between the pre and post treatment is 46.7%, 53.3%, 0% and -100%.
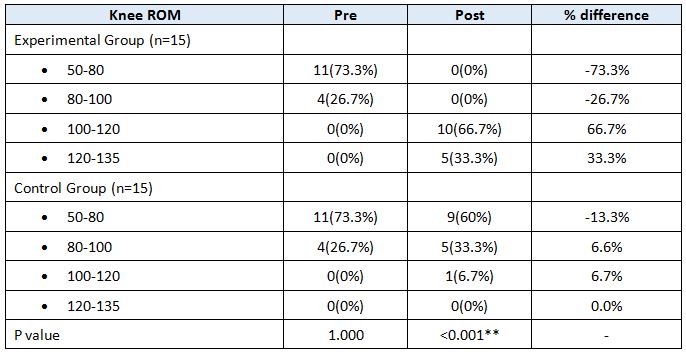
In table 4, Knee ROM has been ranged as 50-80, 80-100,100-120,120-135 degree. The % difference between pre and post treatment is -73.3%,-26.7%, 66.7%, and 33.3% which shows the high significance of the treatment in Experimental Group. The P value is of <0.001** resulting highly significant. In control Group, the KROM in day 14 is 60%, 33.3%, 6.7%, 0% respectively for the given ROM range which indicates that there is very less improvement in KROM after treatment. The mean difference is not as high as that of experimental Group which is -13%, 6.6%, 6.7% and 0.0% respectively for the given range.
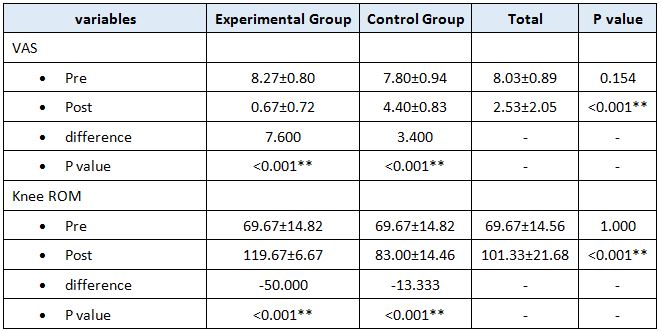
In table 5, VAS score of the patient in EC was 8.27±0.80 whereas post treatment in day 14 it became 0.67±0.72. The mean difference noted is 7.600 and the p value is highly significant at <0.001**. Similarly for control group, VAS score in day 1 is 7.80±0.94 and for day 14 is 4.40±0.83. There is not much difference between pre and post score for VAS in control group, which is just 3.400.
Knee ROM for EC in day 1 was 69.67±14.82 whereas in day 14 it is 119.67±6.67.The mean difference between pre and post treatment score is of -50.000 and the P value at <0.001**. However, control group doesn’t depict much change after treatment. The mean difference between Pre and Post treatment score is just -13.333, far less than that we achieved in EC.

Table 6 displays the difference in VAS and Knee ROM of patients of. Experimental group and control group. Difference in VAS score is 5.50±2.42 and Knee ROM is 31.67±22.18.
DISCUSSION
The purpose of the study was to find the effectiveness of iontophoresis with open kinematic chain exercises to reduce pain and to increase knee ROM in sports person with pes anserine bursitis. The study consists of 30 sports persons diagnosed with Pes Anserine bursitis.15 subjects were kept in experimental group and other 15 in control group. The subjects in experimental group received iontophoresis with open kinematic chain exercises of knee and the control group was treated with ultrasound only. In this study, experimental group and control group result were analysed using student t test and chi square test.
Result obtained from this present study shows that when the mean reduction values of VAS and ROM were analyzed within the groups, it was statistically significant in both the groups for VAS score whereas there was no any effect in KROM in control group. Iontophoresis along with open kinematic chain exercises was found to be very effective in reducing pain and improving ROM. VAS score assessment for pain showed significant improvement in both the groups after the treatment.
This statement is supported by Robert et al (2003) where they concluded that iontophoresis administration of Dexa-methasone sodium phosphate is well tolerated by the patients and is able to reduce pain.The statement is further supported by Linda C et al (1995) where dexa-methasone sodium phosphate was used to treat rheumatic arthritis and the result obtained showed that iontophoresis treatment was more effective in reducing pain and improving ROM. The dexamethasone sodium phosphate delivered via iontophoresis penetrates deep into the joint and thus reduces the symptoms 9.
Iontophoresis is the most commonly used method for pain and inflammation. Iontophoresis for treatment of locomotor system lesions should be considered as an alternative to peri and intra-articular injections because the drugs used diffuse to the tissues along the dermal barrier and penetrate into the body and thereby reduces the symptoms more effectively.Iontophoresis administration of dexa-methasone sodium phosphate was more effective in reducing the pain and other symptoms in short term follow up for patients with lateral Epicondylitis.
Although ultrasound was found to be reducing pain and increase the healing process, the result obtained from this study was not as highly significant as in experimental group. Therefore all the above literature supports the efficacy of iontophoresis in reducing the pain and allowing the better tolerance for exercises.The study was designed to find the effectiveness of iontophresis and open kinematic chain exercises to reduce pain and to improve KROM in sports person with Pes anserine Bursitis.
This study was a randomised experimental study where 30 sports person with Pes anserine bursitis of age group 15-30 wereselected.The subjects were evaluated and included for the study using inclusion criteria such as VAS score 6-9, both the gender and tenderness over the pes anserine bursa. Subject with recent surgery in and around the knee, stress fracture, and other progressive neurological deficit were excluded. Subjects who were willing to participate in the study were requested to fill the consent form.
On day one, pre- treatment baseline assessment was done using VAS for pain assessment and knee ROM by using goniometer.30 Subjects were assigned to either group of 15 in each group. That is experimental group (EG) which received iontophoresis and OKC exercises and control group (CG) which received ultrasound therapy. Post treatment assessment was done on 12th day of treatment using VAS and by measuring KROM using goniometer. Data were analysed using Paired –“t” test and Un-paired “t” test. The result shows that there is reduction of pain and improvement in KROM after 12 days of intervention in EG when it is compared to CG.
Therefore the study concludes that the iontophoresis and open kinematic chain exercises are an effective intervention to reduce pain and to increase KROM in sports person with Pes Anserine bursitis after the 12 days of treatment. The analysis found the highly significant differences in between the pre and post test score of KROM for experimental group. This statement is supported by M Seshagirirao et al (2016) which concluded that open kinematic chain exercises are effective in improving the strength and knee function 10.
Graham et al (1993)found that Open kinematic chain exercises are helpful in improving range of motion and strength of quadriceps and hamstrings muscles. This statement is further supported by the study William E Prentice (2003) who observed that open kinematic chain exercises are helpful to gain strength, flexibility and endurance of hamstrings muscles group in sports person affected with Pes Anserine bursitis. Open kinematic chain exercises of knee were studied and the result obtained showed significant improvement in the hamstrings strength and ROM. Therefore all the above literature supports the efficacy of iontophoresis and open kinematic chain exercises in reducing pain and improving knee ROM in sports person with Pes anserine bursitis11.
As Pes anserine bursitis is considered as a self- limiting disorder, in some cases it is not possible to determine if this self-limiting factor led to the improvement of pain levels and knee ROM instead of treatment administered. The sample size is small and the treatment duration is for short period of time. In future, further studies can be done on larger sample size and for long duration. Additionally, further studies can be done which involves treatment programs like iontophoresis and close kinematic chain exercises.
Ethical Clearance: Ethical clearance has obtained from Institute of Neuroscience, Kolkata to conduct this study with reference number: 214/ Research/IRB/2018-19dated 24/09/2019.
Conflicts of Interest: The author declares that there is no competing interest in publishing this article.
Fund for the study: This is self-funded study.
CONCLUSION
This study concluded that the experimental group which received iontophoresis along with open kinematic chain exercises demonstrated good effect in reducing pain and increasing Knee ROM. But when the experimental groups is compared with the control group which received only ultrasound therapy, EG showed significant improvement in VAS and KROM score whereas there is not much significant improvement in outcome measures post treatment in control group.
REFERENCE
- Miller RH III. (1998)Knee injuries. In: Canale ST, ed. Campbell s operative orthopaedics. St Louis: Mosby; 1113–1299. .
- Pompan DC. (2016). Pes Anserine Bursitis: An Underdiagnosed Cause of Knee Pain in Overweight Women. Am Fam Physician. Feb 01; 93(3):170.
- MSeshagiriRao et al. (2016). Effectiveness of open kinematic chain exercises versus closed kinematic chain exercises of knee in meniscal instability athletics. International Journal of Physiotherapy and Research 4(1):1345-1351 ·
- McMorrisy and perry et al, (2005). Effect of open vs close kinematic chain exercises in extensor resistance training in knee injury patient.
- Sim J, Waterfield J. Validity, (1997). Reliability and responsiveness in the assessment of pain. Physiotherapy theory and Practice; 13: 23-27.
- Revill S, Robinson J, Ronsen M and Hogg M. (1976).The reliability of a linear analogue for evaluating pain.Anaes; 31:1191-1198.
- Gogia PP, Braatz JH, Rose SJ, Norton BJ. (1987). Reliability and validity of goniometric measurements at the knee. 67(2):192-5.
- Escamilla RF,Fleising GS, Zheng N, Barrentine SW, Wilk KE, Andrews J R. (1998). Medsci sports exercises apr 30; (4).
- Lysholm J, Gillquist J. (1982). Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med 3; (10): 150-4.
- Neeter C, Thomee R, Silbernager KG, et al. (2003). Iontophoresis with or without dexamethasone in the treatment of acutachilles tendon pain. Scand J Med Sci Sports; 3:376-382.
| Citation: Gummadi Ashish (2021). A study to find the effectiveness of iontophoresis with open kinematic chain exercises in Pes Anserine bursitis in sports persons, ijmaes; 7 (1); 916-926. |
Leave a Reply