
INTERNATIONAL JOURNAL OF MEDICAL AND EXERCISE SCIENCE
Efficacy of selective trunk activity in improving trunk control in hemiplegic patients
Manjunatha. H 1, Jibi Paul 2, Madan Mohan.M.R3
Corresponding Author:
1Principal, East Point College of Physiotherapy, Jnana Prabha, Bidarahalli, Virgo Nagar, Bangalore, India, Mail id: manjuinlife@gmail.com
Co Authors:
2Professor, Faculty of Physiotherapy, DR MGR Educational and Research Institute, Velappanchavadi, Chennai,India
3Associate Professor East Point College of Physiotherapy, Jnana Prabha, Bidarahalli, Virgo Nagar, Bangalore, India.
ABSTRACT
Background and objective: Trunk control is a crucial component to perform motor function and also to maintain good posture. Trunk gives background for moving upper limbs and lower limbs. The objective of this study was to find out the effectiveness of selective trunk activities in rehabilitation of hemiplegia.
Methods: It is a pre and post experimental design. 30 patients have participated and were divided into two equal groups. i.e, experimental and control group, with 15 subjects in each group. Experimental group received routine neuro-rehabilitation along with selective trunk activities, whereas, control group received only routine neuro-rehabilitation program. Pre and post assessment of trunk balance and impairment was measured by using Trunk Impairment Scale (TIS) and Rivermead Motor Assessment Protocol (RMAP).
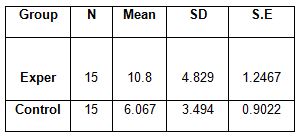
Results: Before the treatment mean values of both control and experimental groups were approximately equivalent There was a significant increase in the mean value of the TIS and RMAP in the experimental group than that of the control group.
Conclusion: Posture and stability are the key factors in maintaining proper balance of the trunk. Hence, selective trunk activity has a significant improvement in trunk balance and postural stability and could be considered as an important part in rehabilitation of hemiplegia.
Keywords: Hemiplegia, trunk movements, selective trunk activity, stroke, postural stability, balance.
Received on 11th April 2019, Revised on 10th May 2019, Accepted on 28th May 2019
INTRODUCTION
Stroke is one of the leading causes of adult disability resulting in chronic neurological deficits. Of the neurological sequelae that produce persistent functional disability, hemiparesis/hemiplegia is the most common. Stroke has a major impact on patient’s life. The sudden loss of any capacity of a person can cause severe stress, not only to the patient but also to the whole family 1, 2.
A stroke or cerebrovascular accident results in sudden specific neurological deficits. It is the suddenness of this neurological deficit occurring over seconds, minutes, hours or few days that characterize the disorder of vascular system 3.
Among all the neurological diseases of adult life, the cerebrovascular ones clearly rank first in frequency and importance. At least 50% of neurological disorders in a general hospital are of this type (Maurice Victor and Allen.H-Ropper)4.
Hemiplegia, a paralysis of one side of the body, is the classical sign of neurovascular disease of the brain. It is one of the many manifestations of neurovascular disease and it occurs with strokes involving the cerebral hemisphere or the brain stem 5.
Incidence, Prevalence And General Prognosis: Stroke is the third major cause of death in worldwide; the worldwide incidence has been quoted as 2 per 1000 population per annum; about 4/1000 in the people aged 45-84 years6.
In India the incidence of cerebro-vascular disease was found to be 13/100,000 population per year in a study conducted at Vellore in 1969-1971, and 33/100,000/year in a study conducted at Rohtak. A WHO study in 1990 quoted incidence of mortality due to stroke in India to be 73/100,000/year7.
The survival, recovery and ultimate out come in stroke patients depend on various variables, out of which important ones are demographic, underlying medical disorders related, lesion related and specific therapy related 8.
Most patients who survive an acute ischaemic or hemorrhagic stroke have at least some lessening of their neurologic impairments and related functional disabilities in subsequent 3-12 months. The mechanisms that permit improvements make a way to understand. Clinicians can potentially manipulate these basic mechanisms with biological rehabilitative interventions that enhance recovery of function 9, 10.
Neuroplasticity: The most informative studies on neuroplasticity are those that have been specifically directed towards defining changes induced by learning. One approach has been documented about the pattern of distributed neural response representation of specific inputs before and after learning. In particular neural responses have been measured in the primary auditory, somatosensory, and motor cortices in animals. These animal studies have commonly been paired with behavioral studies in humans. Especially when considered together, these animal and human studies provide strong inference about the ability of the brain to functionally self-organize, during development, but also in adulthood, as well as after injury.
Problems associated with hemiplegia: In rehabilitation of patients who have suffered a stroke or some other unilateral brain lesion there is a widespread tendency to focus attention only on those problems, which can actually be seen. Observing the patient, the therapist immediately notices the problem of his spastic arm, his inability to move his fingers or use his hand 11.
Jimenez and Morgan (1979) gave a figure of only 59%of patients with a stroke who were able to care for themselves independently when they were discharged from hospital 12.
Problems due to lack of trunk movements: Lack of proximal stabilization influences the limbs profoundly, in that, the arm and leg can only be moved in spastic synergies. Distal spasticity is further increased as the patient tries to compensate for the loss of fixation when he attempts to move against gravity 13.
The abdominal muscles on the non paretic side are affected as well, although not so drastically, due to the fact that no stable insertion is provided by the aponeurosis. As Perkins and Kent (1986), explaining the action of the transverse abdominals and obliques write, “Because all of these muscles are paired, when contracted, they pull in tug-of-war fashion on opposite sides of the abdominal aponeurosis”.
Loss of selective activity in the various muscle groups of the trunk means that the patient is unable to stabilize his thoracic spine in extension while using his lower abdominal muscles (flexors) in isolation, as in walking, for example, neither can be maintained in extension when using the abdominal muscles unilaterally for side flexion of the trunk nor to rotate the side forward 14.
Objectives of the study: To use the selective trunk activity and to find out its efficacy in maintaining the proper balance of a trunk in hemiplegics and also to make the trunk area fit enough to be able to function.
METHODOLODY
Study design: Designing of a study is almost like planning, executing and analyzing a particular population on the basis of their relationship being established between and among the variable of the population. The present study we considered before and after designing system, which is called ‘Pretest Posttest control group design’. The effect was measured both before and after the exposure of the independent variable in the experiment.
Sample size: Total number of subjects for the study is 30. In total 37 cases considered for the study, out of that 5 dropped out of the study due to personal reasons and 2 died during the course of treatment, remaining 30 cases were subjected for the study.
They are divided into 2 equal groups, 15 in each group. Group A: Control group 15 subjects (Males-9, Females-6). Group B: Experimental group 15 subjects (Males-10, Females-5)
Sampling method: For the sake of study the subjects were randomly selected. The first case were allotted to the experimental group and second for the control group, in the same manner third case for experimental group and fourth for control group till the number of cases required for the study were collected, in between, as mentioned earlier 7 cases were deleted from the list, only 30 were considered.
Inclusion criteria: Patients who can able to perform Brunnstrom’s recovery stage 2nd and onwards, Both sexes, Age group between 45 to 65years.
Exclusion criteria: Hemiplegia due to other than vascular causes like traumatic, brain tumors etc.,Hemiplegia with other neurological impairment, psychiatric problems and acute heart diseases.
Source of sample: Subjects are taken from In-patient and outpatient department of Manipal Hospital Bangalore. Outpatient department NIMHANS Hospital Bangalore. Out-patient department Garden City College Of Physiotherapy, Bangalare.
Duration Of The Study: Total duration of the study was three months. In the first 45 days 15 cases including both the groups were treated, next 45 days another 15 cases including both the groups were treated.
Procedure: In charges of the department in various hospitals are explained regarding the study for obtaining permission and notice is given in stroke units, asking hemiplegics to be volunteer. Before the patients were subjected for the independent program their social-demographic factor, clinical history, etiological factor, present signs and symptoms and their report of the neurologist including the radiological examination were noted down.
The patients then were subjected to the module of treatment strategies, in different setting. Some time alternate or sometime daily based on the availability and convenient of the patient.
The group-A received routine neuro- rehabilitation program which include passive limb physiotherapy, voluntary control re-education program for upper limb and lower limb, balance retraining program and gait re-education program. The subject under group-B underwent all the above-mentioned therapeutic program along with selective trunk activity program was administered.
When the patient has little control over the movement in his trunk, he can practice activity in lying and sitting in preparation for moving against gravity. The therapist is ensures that movements are carried accurately and economically.
The therapist should give the patient adequate support at all times as he will otherwise exert himself too much and as a result distal spasticity will increase. Care must be taken to ensure that the patient does not use compensatory movements, which he will do if the activity is too difficult for him.
Selective trunk activities that have been given to the patients as proposed by Patricia M Davies (1980) are: Reaching forward to reach the floor, Transferring the weight sideways, Trunk rotation with flexion, Active side flexion, Moving the trunk forward and backwards.
Selective lateral flexion of the lumbar spine with little help in stabilizing the thorax, Selective side flexion of lower trunk with one leg crossed over other, Moving the elbows sideways to reach the treatment table etc..Before the treatment both the groups were assessed for the trunk balance by using Trunk impairment scale [TIS], Rivermead motor assessment protocol[RMA],
Post treatment assessments were made again by using the same tools. Both pre and post assessments of control and experimental groups were taken for calculation and data analysis.


RESULTS
Thirty subjects were included in this study, who were assigned into two groups- Group A and Group-B. The gender distribution in Group A is 10 males and 5 females, whereas in Group B is 9 males and 6 females.
The group-A received routine neuro rehabilitation program which includes passive limb physiotherapy, voluntary control reeducation program for upper limb and lower limb, balance retraining program and gait reeducation. The subjects under Group B underwent the entire above-mentioned therapeutic program along with selective trunk activity program.
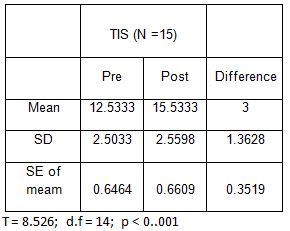
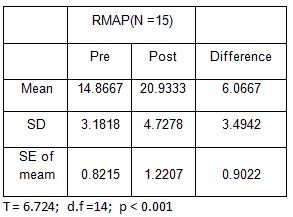
Control group:
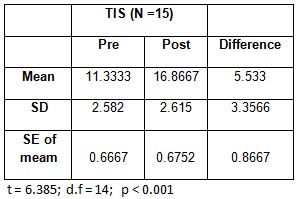
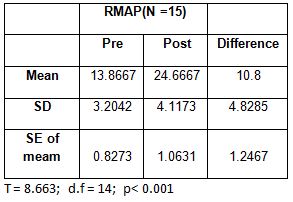
Experimental group:
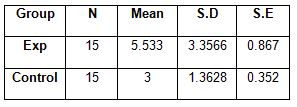
Levene’s Test for Equality of Variances: F = 8.181; d.f =1.29; p < 0.01 Equality of Variances assumed: Student t = 2.708 d.f = 28; p < 0.02.
DISCUSSION
The current study combined routine physiotherapy with the selective trunk activity for one group and routine physiotherapy alone for the other group. The significant improvement in the trunk control of the hemiplegic patients in the experimental group, measured by TIS and RMAP, has strongly proved the effectiveness of selective trunk activity program. Thus, rehabilitation of hemiplegic patients should focus on enhancing the activation of selected trunk muscles and there by improving both the anticipatory and postural strategies 15.
In a study conducted by Ruth Dickstein et al in 1998, activation of selected trunk muscles during symmetric functional activities was evaluated in hemiplegic patients. They documented that the impairment of trunk control in hemiplegic patients, results in asymmetry of rotatory and side bending activities. They also found that the symmetric trunk activities depend on the normal function of the abdominal axial muscles. In conclusion, they recommended for further research to determine the role of trunk muscles in broad repertoire of activities and thus to plan efficient rehabilitation strategies 16, 17.
Earlier in 2002, Marianne De Seze et al had suggested voluntary control retraining of trunk combined with special exploration task to improve the postural control of hemiplegic patient 18.
Postural disturbances are frequent in victims of hemiplegia and limit or delay the recovery of other motor strategies and functional independence. This makes postural control a priority in post stroke rehabilitation 19.
CONCLUSION
The importance of selective trunk activity in the rehabilitation of the hemiplegic patient has been grossly underestimated. The loss of such selective activity has not been fully realized.
This study, in this connection, discusses the selective trunk activity and tries to find out its efficacy in maintaining the proper balance of trunk in hemiplegics, so as to make the trunk area fit enough to be able to function. Consequently, to plan certain interventional strategies as well as rehabilitative measures for the same is important.
In conclusion, this study enunciates that; the selective trunk activity is prima-facie aspect of the hemiplegic rehabilitative rationale for obtaining a desired outcome.
Limitation: Study was not done on particular side of the lesion. Study duration was less, effective improvement can be seen in longer duration of Neurorehabilitaton.
Recommendation: Studies can be done on large samples. Selection of patients was by Brunnstroms recovery stages. Although it has less validity.
REFERENCES
- Bhalla, O.P.Gupta, S.B.Gupta. Department of medicine MGIMS, Sevagram, wardhan (MS) “Predicting mortality in stroke”, Neurol India 2002, 50: 279-281.
- Warlow CP, Dennis MS, Vanginj J et al: “A practical approach to management of stroke patients, in stroke: a practical guide to management”. Blackwell sciences London. 1996; 360-384.
- D. Nagaraja, S.G. Gurumurthy, A.B. Taly, K. Subbakrishna. “Risk factor for stroke : Relative risk in young and elderly”. Neurology India, 46, 183-184, 1998.
- Prasad K; “Epidemiology of cerebrovascular disorders in India”. in recent concept in stroke by Bansal BC(ed) Indian college of physicians New Delhi 1999: 4; 19.
- Hier DB, Eldstein G: “Deriving clinical prediction rules from stroke outcome research”. 1991, 22; 1431-1436.
- Collen FM, Wade DT, Brandshaw CM, “Mobility after stroke: reliability of measures of impairment and disability. Int Disabil Stud 12:6-9, 1990.
- Langhammer B, Stanghelle J.K,”A comparison of two different approaches of physiotherapy in stroke rehabilitation: a randomized controlled study”, Clin Rehab 14:361-369, 2000.
- Endres M, Nyary I, Banhidi M, Deak G. “Stroke rehabilitation: a method and evaluation; Inter J. Rehabil 13; 225-235, 1990.
- collin FM, Wade DT, Robb GF, Brad shaw CM, “The Rivermead Mobility Index: A further development of the Rivermead Motor assessment”. Int Disabil Stud 13: 50-54, 1991.
- Hoens AM, Telfer MM and Strauss GR: “An isokinetic evaluation of trunk strength in elite female field hockey players”. Australian Journal of Physiotherapy; 1990-36:163-171.
- G Verheyden, ANieuwboer, “The trunk impairment scale : a new tool to measure motor impairment of trunk after stroke”. Clinical rehabilitation 2004; 18: 326-334.
- Richardson CA, Toppenberg R, Jull G: “An initial evaluation of eight abdominal exercises for their ability to provide stabilisation for the lumbar spine”. Australian Journal of Physiotherapy; 1990-36: 6-11.
- Sacklely CM, Lincoln NB, “The Verbal administration of the gross function scale of the Rivermead Motor assessment”. Clinical Rehabilitation; 4;301;303, 1990.
- Dickstein, Ruth DSc; Sheffi, Sara MSc; Haim, Zvika Ben Bsc; Shabtai, Esther MSc; Markovici, Emanuel MD: “Activation of Flexor and Extensor Trunk Muscles in Hemiparesis” American Journal of Physical Medicine & Rehabilitation. 79(3):228-234, May/June 2000.
- Ching-Lin Hsieh, Ching-Fan Sheu PhD. “Trunk control as an Early predictor of Comprehensive activities of Daily living function in stroke patients”. Stroke. 33;2626,2002.
- Ruth Dickstein, DSc, Sara Shefi, MSc, Emanuel Marcovitz, MD, Yael Villa, PhD “Anticipatory Postural Adjustment in Selected Trunk Muscles in Poststroke Hemiparetic Patients” ,Arch Phys Med Rehabil 2004; 85:261-7.
- Dominique van Roon., Bert Steenbergen, Ruud G.J. Meulenbroek. “Trunk use and co-contraction in cerebral palsy as regulatory mechanisms for accuracy control” Neuropsychologia 43 (2005) 497–508
- Sylvie Messier, MSc, OT, Daniel Bourbonnais, PhD, OT, Johanne Desrosiers, PhD, OT, “Dynamic Analysis of Trunk Flexion After Stroke”. Arch Phys, Med Rehabil 2004;85:1619-24.
- Franchignoni FP, Tesio L, Ricupero C, Martino MT. “Trunk control test as an early predictor of stroke reha-bilitation outcome. Stroke” 1997;28:1382–1385.
Citation:
Manjunatha. H, Jibi Paul, Madan Mohan. M. R. (2019). Efficacy of selective trunk activity in improving trunk control in hemiplegic patients, ijmaes, 5(2), 559-566.