
INTERNATIONAL JOURNAL OF MEDICAL AND EXERCISE SCIENCE
Effect of rhythmic auditory cueing over conventional physical therapy among hemiparetic stroke patients on functional improvement of upper extremity
Chitra K1 and Jibi Paul2
Author: 2Department of Physiotherapy, Faculty of Health Sciences, KPJ Healthcare University college, Nilai, Malaysia.
Corresponding author: 1Physiotherapist, Charne Hospital, Bangalore, Karnataka, India, E mail: chitra@gmail.com
Abstract
Background and Objective: Functional recovery and motor control is one of the major concerns in stroke patients with performing activities of daily living. Major objective of the study was to investigate the effectiveness of the BATRAC Technique over the conventional physical therapy alone for functional improvement of upper extremity in hemi paretic stroke patient.
Methods: A random sampling method was used to select patients with Right MCA (Middle Cerebral Artery) stroke. Thirty patients were included and randomly divided into two groups by using lottery method, with fifteen in each group A and B. Group A underwent BATRAC Technique and group B underwent conventional physical therapy .The outcomes were measured by the MAS, STREAM and FMS to find out the functional recovery of the upper limb in stroke patients.
Results: Intra group analysis was done by Wilcoxon rank test and the inter group analysis done by Mann- Whitney test. In intra group analysis, group A, got significant reduction in spasticity and significant improvement in voluntary control & functional activities (P<0.005). Group B who underwent conventional physical therapy also showed significant reduction in spasticity & improvement in voluntary control & functional activities. In Comparison between the groups, group A had more significant improvement in voluntary control and functional activities than group B.
Conclusion: This study concluded that physiotherapy with the use of BATRAC Technique is more effective than conventional physical therapy. Statistically BATRAC Technique was highly significant in enhancing the functional improvement of upper limb in hemipareitic stroke patients with right MCA infarction.
Keywords: Stroke, Middle Cerebral Artery, BATRAC Technique, FMS, STREAM, MAS
Received on 14th July 2015, Revised 29th July 2015, Accepted 14th August 2015
INTRODUCTION
Stroke is a major cause of long term disability1, it is most common cause of disability, it is also known as “APOPLEXY”2. Stroke is a clinical syndrome characterized by rapidly developing clinical signs of focal or global disturbance lasting 24 hours or longer or leading to death with no apparent cause other than of vascular origin. Stroke is also called “brain attack”, a disease of the circulatory system caused by the rupturing or blockage of an artery. The middle cerebral artery (MCA) is by far the largest of the cerebral arteries and is the vessel most commonly affected by cerebrovascular accident3.
The most common characteristics of MCA stroke are contra lateral spastic hemi paresis and sensory loss of the face, upper extremity and lower extremity, with upper limb more affected than lower limb. All the stroke patients won’t regain full function after the stroke.4The incidence of stroke is common in patients younger than 60 years5. Stoke prevalence varies in different regions of country and ranges from 40 to 270/100,000 in rural population and the stroke prevalence rates in urban areas are much lower than in metropolitan cities in India.6, 7
The rhythmic
reaching and retrieving actions using a metronome is used to cue the patients
in BATRAC technique.8 An experimental study of rhythmic facilitation
of gait training for hemiparetic stroke patients has concluded that auditory
cueing has been used successfully to promote gait training in stroke patients.
The RAS was very efficient in improving the gait rehabilitation programme in
stroke patients.9 Rhythmic Auditory Stimulation (RAS) was very
efficient in improving the gait rehabilitation programme in stroke patients
tested the patients who had chronic motor impairment following stroke, using
specific rehabilitation therapy that improves arm function. It is usually given
to enhance functional motor recovery and some studies has shown that specific
rehabilitation training will improve motor function in hemi paretic arm of
stroke patients.10
A study on stroke patients reported that Inter- rater reliability of manual tests on elbow flexor spasticity graded by Modified Ashworth Scale is a good and reliable test.11, 12 STREAM for evaluating effects of stroke rehabilitation assessment and movement shown changes over time with that of other measures of impairment and disability and concluded that it is useful in clinical practice and research emerge as a measure of choice for the evaluation of different treatment approaches.13, 14, 15
Objectives of the study
The objectives of the study were to find the effect of bilateral upper extremity training with rhythmic auditory cueing technique to enhance functional improvement of upper limb in hemi paretic stroke patients. Find the effect of conventional physiotherapy to enhance the functional improvement of upper limb in hemi paretic stroke patients. Also to compare the effect of Bilateral upper extremity training with rhythmic auditory cueing technique over conventional physical therapy to enhance functional improvement of upper limb in hemi paretic stroke patients.
MATERIALS AND METHODS
Population of this study included subjects of both genders with MCA stroke and age group between 40-60 years. The study was conducted in the Department of Physiotherapy, Florence Rehabilitation Centre, Kalyan Nagar, Bangalore. Samples were screened from MCA stroke patients referred by physicians with upper limb dysfunction. Patients satisfied the selection criteria were included for the study. Samples included 24 male and 16 female subjects, out of these 5 patients had cognitive deterioration, 3 of them were not willing to participate in the study and 2 patients had musculo-skeletal impairments. Overall 30 patients met the inclusion criteria and were willing to participate in the study. Selected subjects were randomly divided into two groups by using lottery method, with 15 in each. Random sampling method was used to select the subjects so that each and every unit in the population has an equal probability of being selected in the sample. Group A comprised of 8 male and 7 female subjects. Subjects’ in-group A was treated using BATRAC technique. Group B comprised of 6 male and 9 female subjects. These subjects were treated with conventional physical therapy.
Selection criteria included were subjects diagnosed as Right MCA infarction with left hemi paresis, subjects with score of 20 or more than 20 score in STREAM assessment, subjects with spasticity grade less than 2 in Modified Ashworth Scale. Subjects excluded were with chronic stroke, disoriented subjects with stroke, hemorrhagic stroke and stroke due to progressive lesion like tumors, stroke due to traumatic lesion, and subjects with scores more than 2 in MAS.
Selection of Tools: Modified Ashworth Scale (MAS) was selected to assess the muscle spasticity level, the reliability and validity of the scale is good. In MAS the grade 0 indicates no increase in muscle tone and grade 5 indicates affected part(s) rigid in flexion or extension.16 Stroke Rehabilitation Assessment of Movement (STREAM) used to evaluate the level of voluntary motor control for stroke patients. The reliability of the STREAM scores was demonstrated by generalizability coefficients of .99 for total scores and of .96 to .99 for subscale scores. The internal consistency of STREAM score was greater than .98 on the subscales and overall.17 Fugl Meyer scale; this tool was selected for this to evaluate the functional improvement. Fugl Meyer scale was selected because its score is reliable and good for assessing the motor functional level, it has showed very high inter- rater and test- retest reliability with the score.18,19 Materials Used for the study were Stop watch / timer, Paper, Pen, Reflex hammer, Table, Low couch, Chair and BATRAC Machine.
RESULTS
The variation of the change in the values from pre-test to post-test within the experimental and control groups in case of the three different scales are compared using Wilcoxon signed rank test. The variation of change in the values from pre-test to post-test between experimental and control group in case of all the three different scales are compared using Mann-Whitney test. The difference is considered statistically significant whenever p≤0.05.
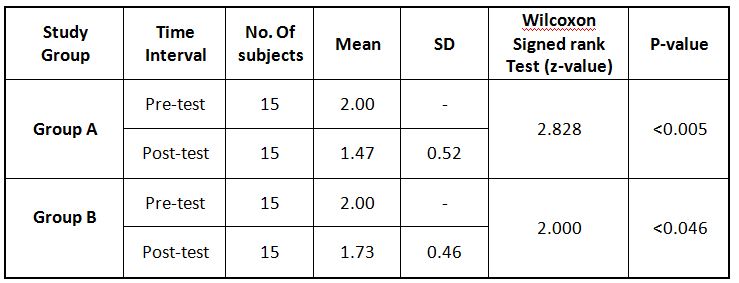
The study indicated that there is significant reduction in spasticity in both the groups. When compared among the groups, group A shows more reduction in spasticity than group B (Table-1).
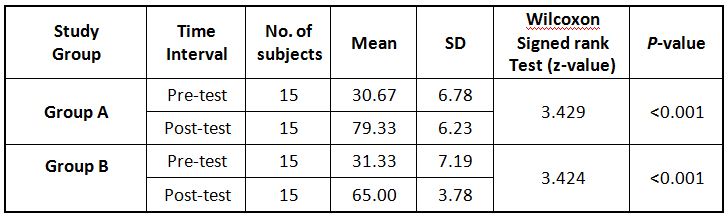
The study demonstrated that both group got significant improvement in voluntary control; group A has more improvement compared to the group B (Table-2).
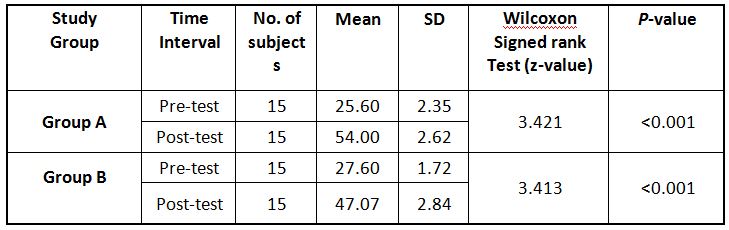
The study showed that both group got significant improvement in functional activities; group A has more improvement compared to the group B (Table-3).
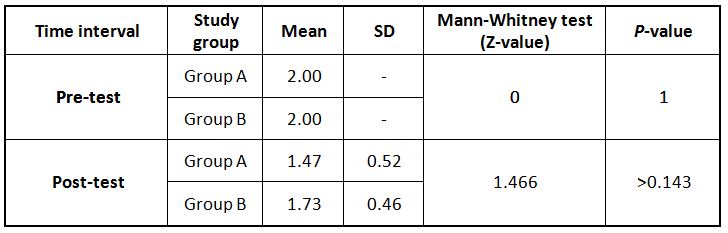
The study observed that statistically there is no significant difference between Group A and B in reduction of spasticity during pre and post-test (Table-4).
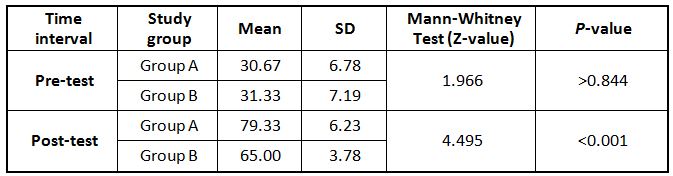
Table 5 Comparison between the groups of STREAM Scale using Mann-Whitney test
The study noticed that statistically there is no significant difference between Group A and B during pretest in improvement of voluntary control but there is high significant during post-test (Table-5).
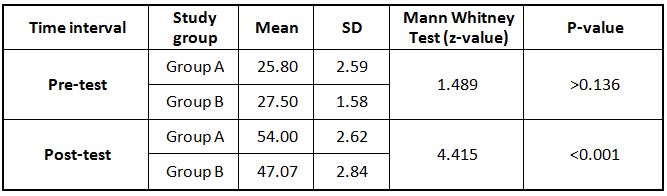
The study observed that statistically there is no significant difference between Group A and B during pretest in improvement of functional activity but there is high significant during post-test (Table-6).
DISCUSSION
Bilateral arm training with rhythmic auditory cueing (BATRAC) improves motor cortex activation and function in chronic stoke more than do standardized dose-matched therapeutic exercises. 20, 21The 4study has stated that Patients who had BATRAC therapy were more likely to have changes in their brain, including in the areas that control voluntary movement, and were more likely to regain function in their affected arm and also reported that BATRAC therapy can help people who have lost partial movement in an arm 22, 23 .
The individual effects of BATRAC technique over conventional physical therapy were analyzed with regard to spasticity, voluntary activity and functional recovery of the upper extremity. Wilcoxon signed ranks test, and Mann Whitney test were used to analyse the data to find the significance of Fugl Meyer scale MAS, STREAM between and within the two groups.
The inter group analysis between the groups of STREAM scale shows no statistical significance in pre-test (Z=1.966, p>0.844). After the treatment shows statistical significance in post-test (Z=4.495, p<0.001), which implies that group B, has less mean than group A. In this study BATRAC show better improvement in voluntary control than Conventional physical therapy. The inter group analysis between the groups of FMS shows no statistical significance in pre-test (Z=1.489, p>0.136). After the treatment shows statistical significance in post test (Z=4.415, p<0.001). The study implies that group B has less mean than group A. BATRAC in this study demonstrated better improvement in functional activities than Conventional physical therapy.
CONCLUSION
Hemi paresis is a leading cause of functional disability after stroke. Therefore some special attention is needed for the functional recovery in stroke. MCA stroke particularly needs more specific exercises to improve functional ability of upper limb.
The study concluded that the use BATRAC technique is more effective than Conventional physiotherapy on functional recovery in stroke patient. BATRAC technique can bring out significant improvement in functional activity of upper limb in right MCA stroke.
REFERENCES
- Dhamija RK, Dhamija SB. Prevalence of stroke in rural community. An overview of Indian experience, J Assoc Physicians India – 1998 Apr; 46(4): 351-4.
- David S Liebeskind. Case fatality rates after hospital admission for stroke BMJ 2003 17 May; 326:1085-1086.
- N S Ward. Mechanisms underlying recovery of motor function after stroke Postgraduate Medical Journal. Jan 2005; 81:510-514.
- Beckman JA, Creager, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA 2002; 288(8): 955.
- Nanette K, Wenger L, Speroff, B. Packard. Stroke and women Le jack Communications publishing company 1993; 313-318.
- D Inzitari et al. The causes and risk of stroke in patients with a symptomatic internal- carotid-artery stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med 2000; 342: 1693-700.
- Tapas Kumar Banerjee, Shymal kumar Das. Epidemiology of stroke in India National Neurosciences centre Calcutta, Kolkata, Bangur institute of neurology, Kolkata, India. Neurology Asia 2006 June 11; 1-4pp.
- Jill Whitall, et al. original contribution of Repetitive Bilateral Arm Training with Rhythmic Auditory Cueing Improves Motor Function in Chronic Hemi paretic Stroke. Copyright in American Heart Association, In Stroke 2000; 31:2390-2395.
- Thaut MH, Mc Intosh GC, Rice RR. Rhythmic facilitation of gait training in hemi paretic stroke rehabilitation 1997 Oct 22; 151(2): 207-
- Birgitta Langhammer, Johan K Stanghelle. Bobath or Motor Relearning Programme? A comparison of two different approaches of physiotherapy in stroke rehabilitation: a randomized control trail. Clinical rehabilitation 2000 February; 14: 361-369.
- Blackburn M, van Vliet P Mockett SP. Reliability of measurements obtained with the modified Ashworth scale in the lower extremities of people with stroke. Phys Ther.2002 Jan; 82(1); 25-34.
- Bohannon RW, Smith MB. Inter rater reliability of a Modified Ashworth Scale of muscle spasticity. Phys Ther. Feb 1987; 67 (2): 206-7.
- Kathy Daley, Nancy mayo, Sharon Wood- Dauphinee. Reliability of Scores on the Stroke Rehabilitation Assessment of Movement (STREAM) Measure. Phys Ther. 1998; 78:8-23.
- Sara Ahmed et al. The Stroke Rehabilitation Assessment of Movement (STREAM): A Comparison With Other Measures Used to Evaluate Effects of Stroke and Rehabilitation Phys Ther Vol. 83, No. 7, July 2003; 617-630 pp.
- Nadina B et al. Randomized controlled trial to evaluated increased intensity of physiotherapy treatment of arm function after stroke. American Heart Association Inc.1999; 30:573-579.
- Gregson J M, Leathley M, Moore A P, Sharma A K, Smith T L, Watkins C L, Reliability of the Tone Assessment Scale and the modified Ashworth scale as clinical tools for assessing post stroke spasticity. Arch Phys Med Rehab 1999 Sep; 80(9):1013-6.
- Wang Chun- Hou et al. Inter-rater reliability and validity of the stroke rehabilitation assessment of movement (STREAM) instrument Journal of rehabilitation medicine. 2002; vol. 34, 20-24 pp.
- Platz T, Pinkowski C Van Wijki C. Reliability and Validity of arm Function assessment with standardized guidelines for the fugl meyer test, Action research arm test and Box and Block test: A multi centre study 2003 Oct; 74(10): 841-9.
- David J. Gladstone, Cynthia J. Danells Sandra E. Black. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties neuro rehabilitation and Neuro Repair. American Society of Neuro rehabilitation. 2002; Vol.16, No.3, 232-240.
- Andreas R. Luft. Repetitive Bilateral Arm Training and Motor Cortex Activation in Chronic Stroke A Randomized Controlled Trial JAMA. 2004 October 20; 292:1853- 1861.
- Laurie Barclay. Bilateral Arm Training With Rhythmic Auditory Cueing Helpful in Chronic Stroke, Med scape medical news, JAMA 2004; 292:1853-1861.
- Francesca Morganti et al. Grasping Virtual Objects: a Feasibility Study for an Inactive Interface Application in stroke, Psychology Journal, 2006; Volume 4, 181-197pp.
- Andreas R. Luft, et al. Repetitive Bilateral Arm Training and Motor Cortex Activation in Chronic Stroke: A Randomized Controlled Trial, JAMA, October 20, 2004— Vol. 292, No. 15, 1853-1861.
Citation:
Chitra K, Jibi Paul (2015). Effect of rhythmic auditory cueing over conventional physical therapy among hemiparetic stroke patients on functional improvement of upper extremity, 2015; 1 (1), 32- 38.