
INTERNATIONAL JOURNAL OF MEDICAL AND EXERCISE SCIENCE
Comparative analgesic effect of Isometric and Isotonic exercises on forearm extensors for lateral epicondylitis of elbow
| Jibi Paul1 , Kousalya. P2 |
| Corresponding Author: 2Student , Faculty of Physiotherapy, Dr.MGR Educational and Research Institute, Chennai, Tamilnadu, India. Mail Id: kousalyapugalenthi3@gmail.com Author: 1Professor, Faculty of Physiotherapy, Dr.MGR Educational and Research Institute, Chennai, Tamilnadu, India. |
ABSTRACT
Background of the study: Tennis Elbow/Lateral Epicondylitis is a work-related pain disorder of common extensor muscles, usually caused by excessive quick repetitive movements of wrist and forearm. The main objective of the study is to find the comparative analgesic effect of isometric and isotonic exercises on forearm extensors for lateral epicondylitis of elbow.
Methodology: This was a comparative study with pre and post intervention.30 subject with tennis elbow were selected based on the inclusion criteria. Further the group was divided into 2 with 15 subjects in each group. The study duration was 4 weeks. Male and female subjects were included in this study. Age group between 30-50 years of age. Group A with 15 subjects were received isometric exercise and Group B with15 subjects received isotonic exercise for a period of 3 sets of 10 repetition for 4 weeks in alternative day. Pain and functional disability were assessed before and after the intervention session using the measurement toolsVAS (Visual analogue scale), andPRTEE (Patient- rated tennis elbow evaluation questionnaire). The special test done for confirming lateral epicondylitis were COZEN’S test and MILL’S TEST.
Result: The result of this study shows that there was significant changes in outcome measures between the Group A (isometric exercise) and Group B (isotonic exercise)with P <0.0001.
Conclusion: The study concluded that isometric exercise is better than isotonic exercise on decreasing the pain and improving the functional activity of patients with lateral epicondylitis of elbow.
Keywords: Isometric exercise, isotonic exercise, Tennis elbow, Visual analogue scale (VAS), Patient-rated tennis elbow evaluation questionnaire (PRTEE).
Received on 23rd August 2019, Revised on 28th August 2019, Accepted on 30th August 2019
INTRODUCTION
Tennis elbow or lateral epicondylitis is one of the most common lesions of arm. Lateral epicondylitis (tennis elbow) is an overuse injury involving the extensor muscles that originate on the lateral epicondylar region of the distal humerus. It is more properly termed a tendinosis that specifically involves the origin of the extensor carpi radialis brevis muscle. It is generally work related or sport related pain disorder of the arm, usually caused by excessive, quick, repetitive movements of wrist and forearm. These quick movements may rupture the proximal attachment of the long extensor muscle and cause local inflammation and pain 1.2,3 .
The degenerative or failed healing tendon response rather than inflammatory. Hence, the increased presence of fibroblast, vascular hyperplasia proteoglycans and glycosaminoglycans together with disorganized and immature collagen may all tale place in the absence of inflammatory cells 4.
The dominant arm is commonly affected with a prevalence of 1-3% in the population, the peak prevalence of tennis elbow is between 30-60 years of age and the disorder appears to be of longer duration and severity in women. The average period of an episode of lateral epicondylitis ranges between six month and two years 5.
Visual analogue scale is considered to be one of the best methods available for the estimation of the intensity of pain. VAS has been found to be easy to administer, highly reliable and valid tool in the clinical measurement of acute and chronic pain6,7.
The PRTEE allows the patients to rate their levels of tennis elbow pain and disability on scale of 0 to 10. It consists of 2 subscales: 1) Pain subscale having 5 items and 2) Functional subscale, in this specific activity having 6 items and usual activities having 4 items. A total score can be computed on a scale of 100 8,9.
Aim of the study: To find the Analgesic effect of isometric exercise and isotonic exercise on forearm extensors and also to compare the effect between isometric exercise and isotonic exercise on forearm extensors of elbow.
METHODOLOGY
This was a comparative study with pre and post intervention.30 subject with tennis elbow were selected based on the inclusion criteria. Further the group was divided into 2 with 15 subjects in each group. The study duration was 4 weeks.
Male and female subjects were included in this study. Age group between 30-50 years of age. Group A with 15 subjects were received isometric exercise and Group B with15 subjects received isotonic exercise for a period of 3 sets of 10 repetition for 4 weeks in alternative day. Subjects with radial nerve compression, fracture, dislocation of elbow, trauma around elbow and ligament injury were excluded from the study.
Pain and functional disability were assessed before and after the intervention session using the measurement toolsVAS (Visual analogue scale), andPRTEE (Patient- rated tennis elbow evaluation questionnaire). The special test done for confirming lateral epicondylitis were COZEN’S test and MILL’S TEST. 30 subjects with lateral epicondylitis were participated in the study. the patient is explained about the treatment procedure both pre and posttest has been analyzed and informed consent was taken from the patients. before start of treatment, the patient was positioned comfortably and assessed thoroughly about his or her condition, shown in the performa. the special test done for confirming lateral epicondylitis are Cozen’s Test and Mill’s Test.
Isometric Exercises: The patient is first relaxed in comfortable position, then the exercise is started with elbow in extension, forearm pronation, wrist in flexion with slight ulnar deviation for extensor carpi radialis brevis tendon. By using the opposite hand to press the stretching hand back towards the subject’s body. This position is hold for 30 sec. Three sets for 10 repetitions at each treatment session in alternative days for 4 weeks and one minute rest between the sets.
Isotonic Exercises: The patient is first
relaxed and seated in comfortable position. The Forearm on the bench, wrist
just beyond edge of bench and grip the dumbbell with palm facing the floor.
Bend the wrist with dumbbell slowly lower the weight, then lift it back up
towards the ceiling. Three sets for 10 repetitions at each treatment session in
alternative days for 4 weeks and one-minute rest between the sets.
Data Analysis and Interpretation:
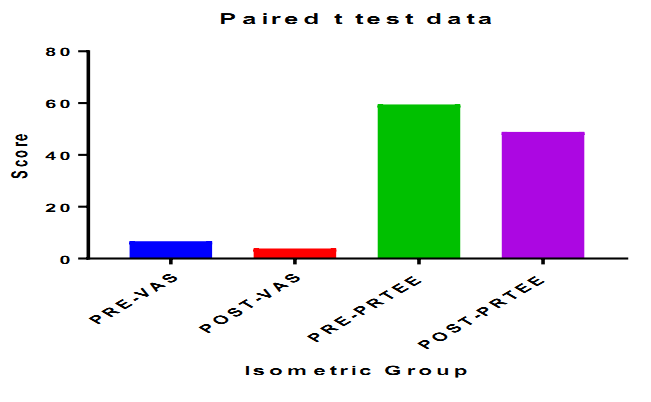
Group A with Isometric Exercise
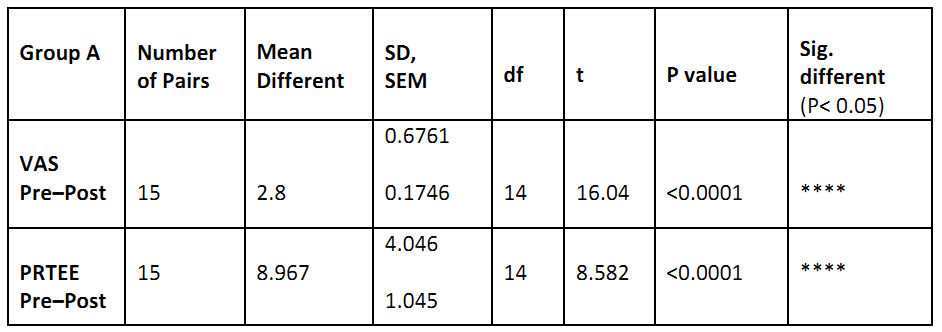
The above table reveals the Mean, standard deviation (SD) t-value, and p-value of the VAS and PRTEE between pre-test and post-test within Group-A (Isometric exercise).
In the VAS score, there is a significant difference between the pre-test and post-test values (P<0.0001).
In the PRTEE, there is a significant difference between the pre-test and post-test values (P <0.0001).
This table shows the statistically difference in VAS, PRTEE between pre-test and post-test values (P<0.0001).
Group B with Isotonic Exercise
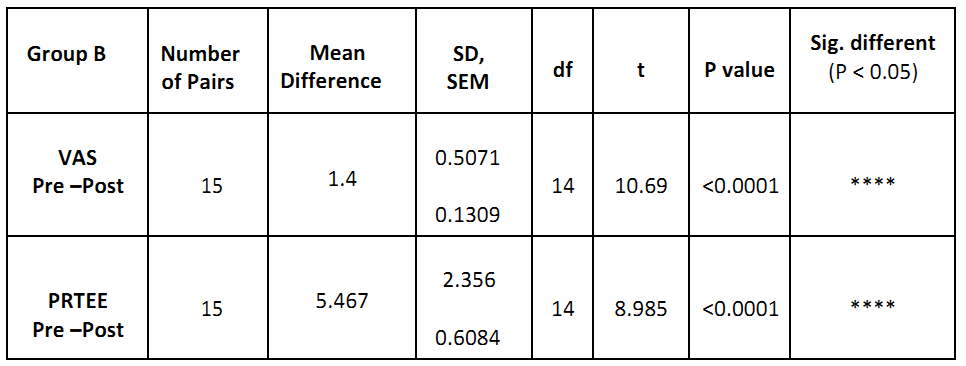
The above table reveals the Mean, standard deviation (SD) t-value, and p-value of the VAS and PRTEE between pre-test and post-test within Group-B (Isotonic exercise).
In the VAS score, there is a significant difference between the pre-test and post-test values (P<0.0001).
In the PRTEE, there is a significant difference between the pre-test and post-test values (P<0.0001).
This table shows the statistically difference in VAS, PRTEE between pre-test and post-test values (P<0.0001).
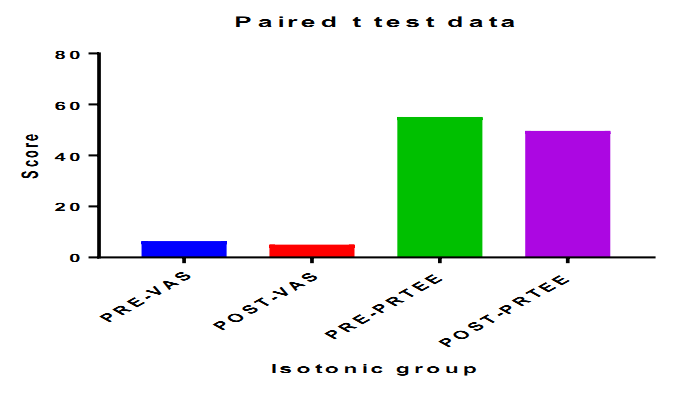
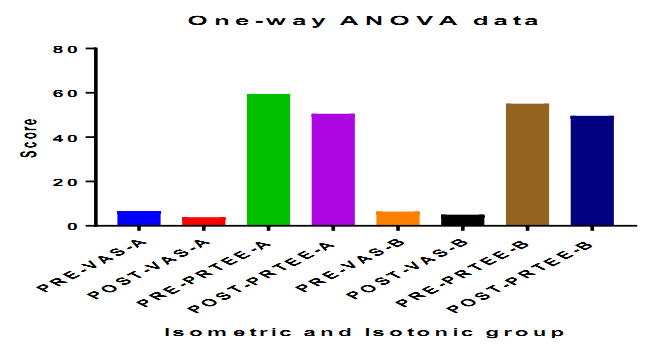
COMPARATIVE STUDY
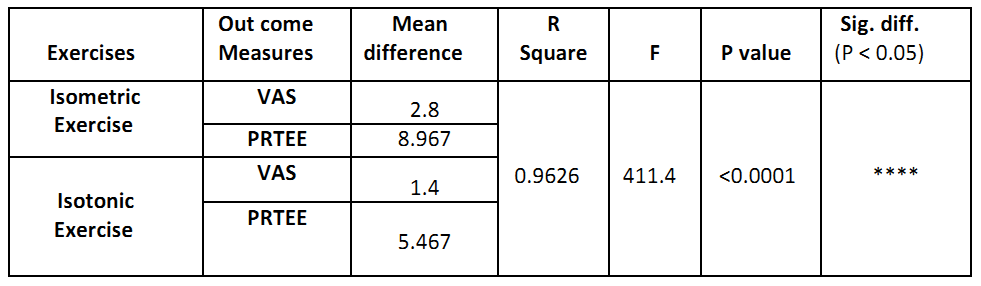
The above table reveals the Mean and p-value of the VAS and PRTEE between the Group A (isometric exercise) & Group B (isotonic group)
This shows significant difference on VAS and PRTEE between Isometric Exercise and Isotonic Exercise group with P value <0.0001.
RESULT
There is a significant difference between the pre-visual analogue scale score (VAS) and post visual analogue scale (VAS) score within Group A & Group B at P≤ 0.0001 where the calculated value is greater than the table value. Hence, the null hypothesis is rejected and accepted the alternative hypothesis.
On comparing mean values between Group A &Group B, on visual analogue scale score (VAS) shows the significant reduction in the post test mean. Group A (isometric exercise) is more effective than Group-B (isotonic exercise) at P≤0.0001, hence the null hypothesis is rejected and accepted the alternative hypothesis.
There is a significant difference between the pre PRTEE score and post PRTEE score within Group A & Group B at P≤ 0.0001 where the calculated value is greater than the table value. Hence, the null hypothesis is rejected and accepted the alternative hypothesis.
On comparing mean values between Group A &Group B on PRTEE score shows the significant reduction in the post test mean. GROUP A (isometric exercise) is more effective than Group-B (isotonic exercise) with P≤0.0001, hence the null hypothesis is rejected and accepted the alternative hypothesis.
DISCUSSION
The study was conducted on 30 subjects with a total of 18 males and 11 females between the age group of 30-50 diagnosed as a case of lateral epicondylitis as per the inclusion criteria. In Group A, (isometric exercise): 15 subjects, 8 males and 6 females. In Group B (isotonic exercise): 15 subjects, 10 males and 5 females. Interventional protocol was of 4 weeks.
To measure this functional disability PRTEE questionnaire was chosen as an outcome measure, according to McDermid (2007), it is primarily subject self-rated perception of pain and functional scale that is a reliable and valid measure of disability. The PRTEE may become the standard primary outcome measures in research of tennis elbow 10,11.
Visual analogue scale is the most commonly used scale to observe the subjective pain therefore it was taken as an outcome measure. A VAS typically consists of 10 cm line. The score equal to 4 or more is considered as moderate pain, a score of 7 or more is considered to be severe pain.
According to Young Park J et al (2010) home-based program of isometric strengthening exercise for the treatment of LET provides a clinically significant improvement [20]. Actually, the mechanism by which a strengthening exercise program causes relief pain remains uncertain12,13.
Most studies regarding the efficacy of exercise investigates eccentric exercise in Achilles tendinopathy. Eccentric strengthening exercise cause tendon strengthening by stimulating mechanoreceptors in tenocytes to produce collagen, which is the key to recovery of tendon injuries. This mechanism produces positive effect in Achilles tendinopathy may not be applicable to LET 14 .
Achilles tendinopathy and lateral epicondylitis are often related to forceful grip activities requiring isometric contraction which would be more beneficial than isotonic contraction in LET15.
Isometric exercise reduced the pain in tendinopathy. Isometric contractions reduce pain in tendon disorders, increasing the strength at the angle of contraction without producing inflammatory signs and increasing the arm function stated by Rio E Kidgell DJ, et al. (2013).
Eccentric training and isometric exercises show diminish pain and improve function, reversing the pathology of tendinopathy in experimental study, which has been stated by R. hawary, W. stanish and W. curwin, (1997.
Isometric exercise program has to carry out without any equipment. but, isotonic often cause increase pain, it should be performed without pain. Execute isotonic exercise with equipment like dumbbell or resistance band necessary.
Group (A) pre-test & post-test mean value for VAS score (2.8) and Group B pre-test& post-test mean value VAS score (1.4) showed a significance difference. Group (A) pre-test& post-test mean value for PRTEE questionnaire (8.967) and Group B pre-test& post-test mean value PRTEE questionnaire (5.467)showed a significance difference.
On based on this background, it may be observed that the Group A (isometric exercise) will be better than Group B (isotonic exercise) for lateral epicondylitis.
The result of study showed that reduction in pain, improvement in functional status was appreciably significant in both the groups. The results obtained from Simple random sampling method following 4 weeks of treatment session indicated that isometric exercise is significantly better than isotonic exercise.
CONCLUSION
This study concluded that the subjects in Group A performing isometric exercise shows more improvement in reducing pain and improving functional activities than in Group B isotonic exercise program in lateral epicondylitis.
Thus, it can be assumed from this study that Group A with Isometric exercise is an effective approach in reducing pain and improving functional activities among lateral Epicondylitis patients.
Ethical Clearance: Ethical clearance has obtained from Faculty of Physiotherapy, DR.MGR Educational and Reasearch Institute, Chennai to conduct this study with reference number: A–030/ PHSIO/ IRB/2018-19dated 07/01/2019.
Conflict of interest: There was no conflict of interest to conduct this study.
Fund for the study: It was aself financed study.
REFERENCE
- De Smedt T, de Jong A, Van Leemput W, Lieven D, Van Glabbeek (2007). Lateral epicondylitis in tennis: update on aetiology, biomechanics and treatment. British journal of sports medicine. Nov
- Haker; lateral epicondylalgia: (1993) Diagnosis, treatment & evaluation; critical reviews in physical & rehabilitation medicine, 5;129-154.
- Jensen K, Di Fabio RP (1989) Evaluation of eccentric exercise in treatment of patellar tendinitis. Phys Ther. 69; 211-216.
- J A (1994) Tennis elbow, Anatomical, epidemiological and therapeutic aspects. Int Orthoepy, 18; 263-267.
- E. P. Roetert, H. Brody, C. J. Dillman, J. L. Groppel, and J. M. (1995). “The biomechanics of tennis elbow: an integrated approach,” Clinics in Sports Medicine, Vol. 14; no. 1; pp. 47-57.
- Pienimäki TT, Tarvainen TK, Siira PT, Vanharanta H. (1996). Progressive strengthening and stretching exercises and ultrasound for chronic lateral Epicondylitis Physiotherapy. 82(9); 522-30.
- S. C. Chen, (1997). “A tennis elbow support,” British Medical Journal, Vol. 2; 6091.
- G. Brattberg, (1983). “Acupuncture therapy for tennis elbow,” Pain, Vol. 16; no. 3; pp. 285-288.
- Molsberger and E. Hille (1994). “The analgesic effect of acupuncture chronic tennis elbow pain,” British Journal of Rheumatology, vol. 33; no. 12; pp. 1162-1165.
- Waugh EJ, Jaglal SB, Davis AM, Tomlinson G, Verrier MC, et al. (2004) Factors associated with prognosis of lateral epicondylitis after 8 weeks of physical therapy. Arch Phys Med Rehab. 85; 308-318.
- Bisset L, Vicenin B (2015) Physiotherapy management of lateral epicondylalgia. J Physio the 61(4); 174-181.
- Stasinopoulos D, Johnson MI (2004) Treatment/management for tendinopathy. Time to abandon the ‘tendinitis’ myth. BMJ 324; 626.
- Raman J, McDermid JC, Grewal R (2012) Effectiveness of different methods of resistance exercises in lateral epicondylosis-a systematic review. J Hand Therapy ;25(1); 5-25.
- Rio E, Kidgell D, Purdam C, Gaida J, Moseley GL, et al. (2015) Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. Br J Sports Med.; 49(19); 1277-1283.
- Young Park J, Park H, Choi J, Sun M, Soo K, et al. (2010) Prospective evaluation of the effectiveness of a home-based program of isometric strengthening exercises: A 12 month follow up. Clinics in orthopaedic surgery. 2(3); 173-178.1;41(11); 816.
Citation:
Jibi Paul, Kousalya. P (2019).Comparative analgesic effect of isometric and isotonic exercises on forearm extensors for lateral epicondylitis of elbow. IJMAES; 5 (3); 617-624.