
INTERNATIONAL JOURNAL OF MEDICAL AND EXERCISE SCIENCE
A study to analyze the effects of global postural re-education method on pulmonary function and thoracic expansion in individuals with moderate chronic obstructive pulmonary disease
| ISHWARYA VARDHINI C1, DENNIS ROBINSON2, JIBI PAUL3 |
Corresponding Author:
1Asst.Professor, Faculty of Physiotherapy, Dr. MGR Educational and Research Institute, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India. Mail id: ishphysio@gmail.com
| Authors: 2Professor, Department of Physiotherapy, KG College of Physiotherpy, Coimbatore, Tamilnadu, India. 3Professor, Faculty of Physiotherapy, Dr.MGR. Deemed to be University, Chennai, Tamilnadu, India. |
ABSTRACT
Background of the study: Chronic obstructive pulmonary disease (COPD) is the 5th cause of mortality and morbidity in the world and represents an economic and social burden. Chronic obstructive pulmonary disease is a chronic pulmonary disorder affecting 10%-15% individuals over age of 45 years. Objective of the study is to compare the effect of conventional pulmonary rehabilitation and Global Postural Re-education method on pulmonary function and thoracic expansion in patients with moderate chronic obstructive pulmonary disease.
Methodology: This was an experimental Study of two groups’ with pre-post comparative study design. The study was conducted for a period of six months in the department of Pulmonology, K.G.Hospital and postgraduate research and medical institute, Coimbatore. All adult patients attending the Pulmonology department of the hospital were assessed and selected for the study. A total of 20 patients with moderate chronic obstructive pulmonary disease were selected by random sampling method and were divided into 2 groups A and B. Pulmonary function test (FEV1/FVC) and Thoracic expansion at Axillary and Xiphoid level was measured and recorded. Unpaired ‘t’test used to find the difference between two groups.
Result: T value for FEV1/FVC was 7.313, thoracic expansion was 11.90 and 16.39 at Axillary & Xiphoid respectively between two groups with ‘P’ value <0.05. The study showed that there is a significant difference in improvement of FEV1/FVC ratio and thoracic expansion in Group-B, who underwent Global postural re-education method.
Conclusion: Global postural re-education method is better intervention in the improvement of pulmonary function, thoracic expansion in patients with moderate chronic obstructive pulmonary disease.
Keywords: Chronic Obstructive Pulmonary Disease, Global Postural Re-education (GPR), Pulmonary function, Thoracic expansion.
Received on 3rd August 2019, Revised on 16th August 2019, Accepted on 29th August 2019
INTRODUCTION
Studies suggest that exercises are aimed to improve mobility of chest wall, thoracic mobility and exercise capacity, reduce breathlessness and symptoms of dejection in patients with chronic obstructive pulmonary disease 1.
By 2020 Chronic obstructive pulmonary disease, is predictable to rise to 3rd place as a cause of death and to 5th place as a cause of loss of disability adjusted life years, as per the baseline projections made in global burden of sickness2.
Reported by The European Respiratory Society (ERS) on Chronic obstructive pulmonary disease is, reduced maximum expiratory flow and slow forced emptying of the lungs, which is slowly progressive and mostly irreversible to medical treatment3, 4.
Factors like, increased visceral mass, improper posture, respiratory disease, muscle weakness and aging lead to compromise in the breathing mechanics that arises from shortening of the muscles of respiration, in turn affecting their ability to produce tension. This ultimately decreases working ability of the respiratory musculature leading to deterioration in the overall quality of life5, 6, 7.
The prevalence and death rate due to chronic obstructive pulmonary disease are increasing and proportionately seem to rise in accordance with increase in smoking. Smoking cessation, disease education, early detection, and treatment will be the most benefit against the cause of morbidity and mortality 8, 9 10.
Objective of the study: Find the effectiveness of Global Postural Re-education method and conventional pulmonary rehabilitation on pulmonary function and thoracic expansion in patients with moderate chronic obstructive pulmonary disease. The main objective of the study is to compare the effectiveness of conventional pulmonary rehabilitation and GPR method on pulmonary function and thoracic expansion in patients with moderate chronic obstructive pulmonary disease.
METHODOLOGY
Study was an experimental two group pre-test and post-test study design. Study was conducted for a period of six months in the department of Pulmonology, K.G.Hospital and postgraduate research and medical institute, Coimbatore. All adult patients attending the pulmonology department of the hospital were assessed and selected for the study.
A total of 20 patients with moderate chronic obstructive pulmonary disease were selected by random sampling method and were divided into Group-A and Group-B. Group-A subjects were involved in conventional pulmonary rehabilitation and Group-B patients performed Global postural re-education programme.
Criteria for selection
Inclusive Criteria: Adults patients with moderate Chronic obstructive pulmonary disease, pulmonary function (FEV1: FVC) ranging from 68%-69% with predicted FEV1 of less than 70%, both sexes were included, age group between 45-50 years, patients who were willing to participate, patients with B.M.I ranging from 20-25, patients who have quit smoking.
Exclusive criteria: Patients with severe Chronic obstructive pulmonary disease, patients with associated respiratory complications, patients with cardiac, orthopedic and neurological problems, patients with skin, peripheral vascular diseases and allergies, Individuals who were unable to quit smoking, Individuals on prolonged corticosteroids.
Outcome measures and measurement tools: Pulmonary function was measured by pulmonary function test (FEV1/FVC). Thoracic expansion at the level of Axillary and Xiphoid was measured by inch tape.
Intervention: Conventional pulmonary rehabilitation for group A and Global postural re-education for group B.
Procedure: Subjects with moderate chronic obstructive pulmonary disease were taken for the study. Both the groups were explained about the procedure that has to be done and consent was obtained from them. Pre-test pulmonary function tests and thoracic expansion were measured and the data’s were recorded.
GROUP-A: They were subjected to Conventional pulmonary rehabilitation.
GROUP-B: They were subjected to Global postural re-education method.
Global Postural Re-Education (G.P.R): G.P.R method includes a series of gentle movements that stretches and strengthens the thoracic cage musculature that has become tight or weak from under use. The protocol consists of respiratory muscle stretching in abducted arm and hip. The subjects were given diaphragmatic relaxation manoeuvre in supine lying Prior to the stretching. Stretching applied by sliding pressure with finger tips bilaterally from xiphocostal angle to the ribs.
They were positioned with arms at an angle of 45 degrees to the body, palms facing ceiling, legs apart, hips and knees flexed and soles of feet facing each other. They were asked to inhale and exhale slowly. The legs were straightened, with the spine erected in supine lying position11,14.
Conventional pulmonary rehabilitation: Pulmonary rehabilitation includes instruction on breathing techniques, upper extremity exercise, chest clearance techniques.
Duration and frequency of session: Both the groups received 2 Sessions/week for a period of 6 months. After a period of 6 months, Post-test pulmonary function tests and thoracic expansion were measured and the results were analyzed statistically.
RESULT
Data Analysis and Interpretation
GROUP-A:
The comparative mean values, standard deviation and paired “t” test values of FEV1/FVC ratio for Group-A patients who were subjected to conventional pulmonary rehabilitation.
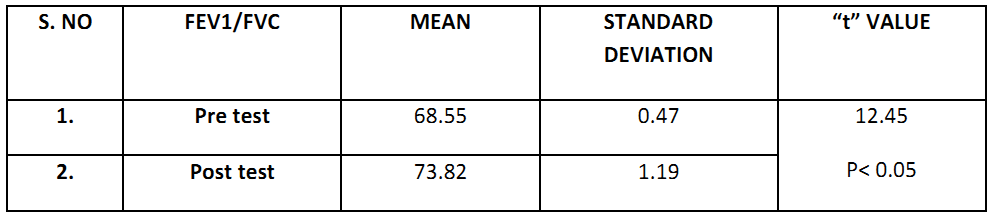
Table 1, shows the analysis of FEV1/FVC ratio on paired “t” test. The‘t’ value for Group –A was 12.45 at 5% significance, which was greater than tabulated‘t’ value 1.83. The result shows major difference in progress of FEV1/FVC ratio between the pre and post test values of GROUP-A.
GROUP-B:
The comparative mean values, standard deviation and paired “t” test values of FEV1/FVC ratio for Group-B patients who were subjected to global postural re-education method.
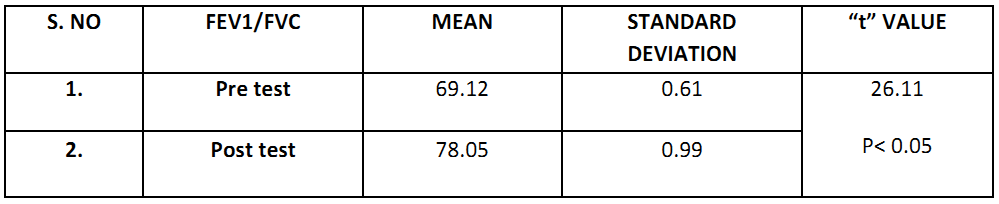
Table 2, shows the analysis of FEV1/FVC ratio on paired “t” test. The‘t’ value for Group –B was 26.11 at 5% significance, which was greater than tabulated ‘t’ value 1.83. T The result shows major difference in progress of FEV1/FVC ratio between the pre and post test values of GROUP-B.
GROUP-A Vs B:
The comparative mean values, standard deviation and unpaired “t” test values of FEV1/FVC ratio for Group-A and B
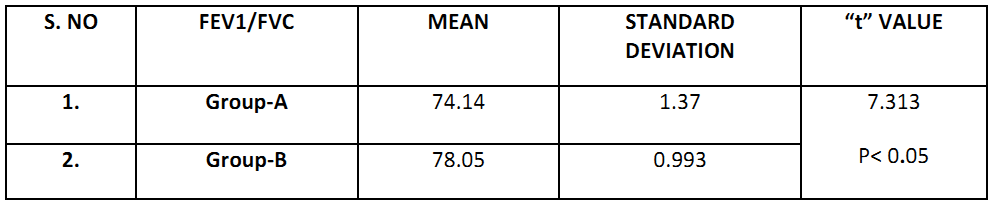
Table 3, shows the analysis of FEV1/FVC ratio on unpaired “t” test. The‘t’ value was 7.313 at 5% significance, which was greater than tabulated ‘t’ value 1.734. The result shows major difference in progress of FEV1/FVC ratio in GROUP-B than GROUP-A. This shows that the study rejects null hypothesis.
GROUP-A:
The comparative mean values, standard deviation and paired “t” test values of thoracic expansion (Axillary) for Group-A patients who were subjected to conventional pulmonary rehabilitation.
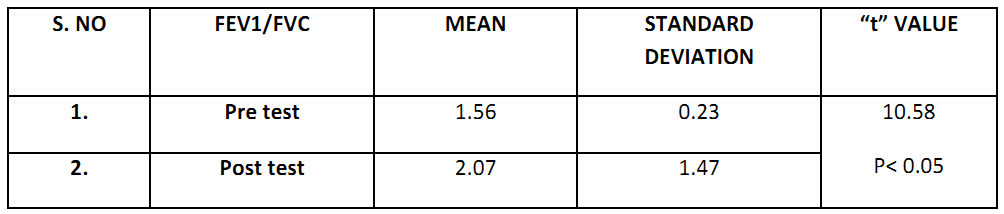
Table 4, shows the analysis of thoracic expansion (Axillary) on paired “t” test. The ‘ t’ value for Group –A was 10.58 at 5% significance, which was greater than tabulated ‘t’ value 1.83. The result shows major difference in progress of thoracic expansion ( Axillary) between pre test and post test values of GROUP-A.
GROUP-B:
The comparative mean values, standard deviation and paired “t” test values of thoracic expansion (Axillary) for Group-B patients who were subjected to Global postural re-education method.
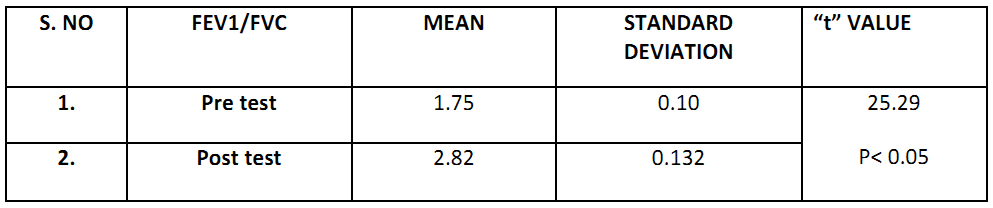
Table 5, shows the analysis of thoracic expansion (Axillary) on paired “t” test. The‘t’ value for Group –B was 25.29 at 5% significance, which was greater than tabulated‘t’ value 1.83. The result shows major difference in progress of thoracic expansion (Axillary) between pre test and post test values of GROUP-B.
GROUP- A Vs B:
The comparative mean values, standard deviation and unpaired “t” test values of thoracic expansion ( Axillary) for Group- A and B.
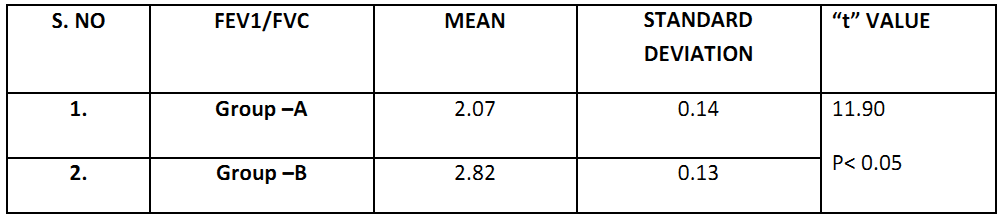
Table 6, shows the analysis of thoracic expansion (Axillary) on unpaired “t” test. The ‘ t’ value for Group-A and B was 11.90 at 5% significance, which was greater than tabulated ‘t’ value 1.734. The result shows major difference in progress of thoracic expansion (Axillary) in GROUP-B than GROUP-A. This shows that the study rejects null hypothesis.
GROUP-A:
The comparative mean values, standard deviation and paired “t” test values of thoracic expansion (Xiphoid) for Group-A patients who were subjected to Conventional pulmonary rehabilitation

Table 7, shows the analysis of thoracic expansion ( Xiphoid ) on paired “t” test. The‘t’ value for Group –A was 6.67 at 5% significance, which was greater than tabulated‘t’ value 1.83. The result shows major difference in progress of thoracic expansion (Xiphoid) between pre test and post test values of GROUP – A .
GROUP-B:
The comparative mean values, standard deviation and paired “t” test values of thoracic expansion (Xiphoid) for Group-B patients who were subjected to Global postural re-education.
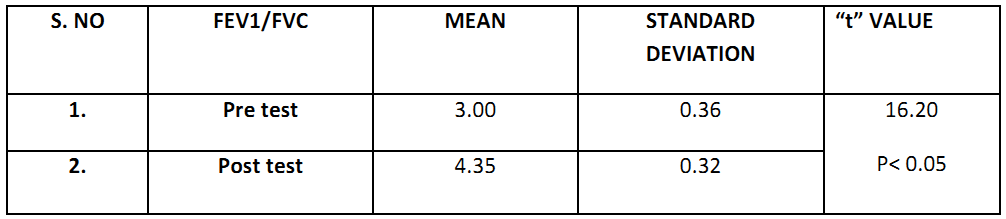
Table 8, shows the analysis of thoracic expansion (Xiphoid) on paired “t” test. The‘t’ value for Group –B was 16.20at 5% significance, which was greater than tabulated‘t’ value 1.83. The result shows major difference in progress of thoracic expansion (Xiphoid) between pre test and post test values of GROUP B.
GROUP- A Vs B:
The comparative mean values, standard deviation and unpaired “t” test values of thoracic expansion ( Xiphoid) for Group- A and B.
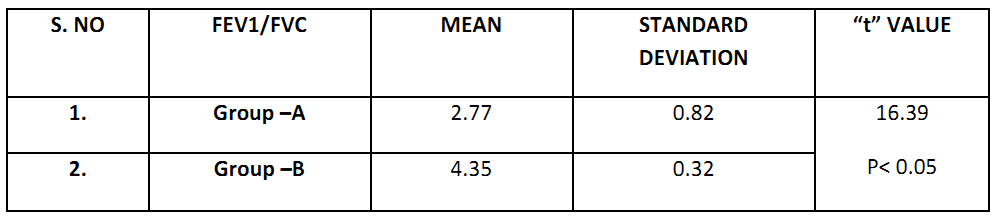
Table 9, shows the analysis of thoracic expansion (Axillary) on unpaired “t” test. The‘t’ value for Group-A and B was 16.39 at 5% significance, which was greater than tabulated‘t’ value 1.73. The result shows major difference in progress of thoracic expansion (Xiphoid) in GROUP-B than GROUP-A. This shows that the Study rejects null hypothesis.
DISCUSSION
This study was aimed to determine the effectiveness of conventional pulmonary rehabilitation and global postural re-education method (G.P.R) on the pulmonary function and thoracic expansion in patients with moderate C.O.P.D. The study’s functional parameters were FEV1/FVC ratio and thoracic expansion (axillary and xiphoid).
A total of 20 patients with moderate COPD (FEV1/FVC ratio of 68% to69% with a predicted FEV1of less than 80%), who fulfilled the selection criteria were randomly selected and divided into two groups containing 10 in each. Group –A received conventional pulmonary rehabilitation and Group-B received G.P.R method. Results obtained from statistical interpretation between group –A & B at 5% level of significance showed major difference in progress of pulmonary function and thoracic expansion in patients with moderate C.O.P.D (t-value-26.11, 25.29, 16.20).
Elaine Paulin et.al,(2003) stated that, that exercises aimed to the increasing mobility of chest wall, improve thoracic mobility and exercise capacity reduce breathlessness and symptoms of depression in patients with chronic obstructive pulmonary disease (Elaine Pauline et.al, 2003)12.
Gossman MR, Rose.S.J(1982), stated that, “When a muscle loses its normal flexibility, there is alteration in length – tension relationship , which in turn reduces the ability of muscle to produce maximum tension ,thereby leading to muscle weakness . The causes for such shortening can be due to various factors like incorrect postural alignment, immobilization of muscle, muscle weakness and aging. Supporting the above study,Katrina, Renita, et al (2008), concluded that, combination of postural exercises and mobilization of soft tissue techniques has positive effects on chest mobility and respiratory muscle strength in chronic obstructive pulmonary disease patients13.
Studies by Derenne JP, Macklem (2007), has stated that, increase in lung volume in chronic obstructive pulmonary disease results in severe shortening of respiratory muscles.This supports the study in the improvements in pulmonary function, thoracic expansion in Group-B patients who underwent G.P.R method which includes stretching and mobilization. Therefore in chronic obstructive pulmonary disease patients, adequate muscle length would increase the efficiency of respiratory muscles, promoting better mechanics of muscles of thoracic wall 14.
According to Souchard P.E (1989), constant contraction of respiratory musculature promotes a particular posture during inspiration, restricting mobility of chest cavity. He also reported excessive shortening of respiratory muscles can result from alterations in respiratory mechanics. Further, Durmus. D, Alavli. G,et al,(2009), stated that, GPR method has major progress than the conventional exercise program in specific pulmonary functions like forced vital capacity, forced volume in 1sec and peak expiratory flow parameters. Maintenance of muscles in lengthened state for a long duration forms the basis of global postural re-education method. In addition, it facilitates alterations that improve in extensibility, elasticity and strength15.
GPR method is effective in increase of thoracic expansion, respiratory muscle strength. Based upon the recommendation suggested by Rosanna et.al, the above study was done and results obtained. Souchard PE (2001, stated that, “GPR uses active muscle stretching postures in which the stretching is made possible by the patient’s participation in isometric contractions in the increasingly Eccentric positions of the shortened muscles16.
Montaldo etal (2000) , stated that, Improvements in expansion of thorax brings marked changes in tension generating capacity of muscles of respiration and reduce the stimulus for control of respiration, thereby reducing breathlessness 17.
Further,Kakisaki etal, (1999), concluded that, an increase in length of muscles of respiration improves expansion of thorax and reduce dyspnoea in patients with chronic obstructive pulmonary disease18.
From the above, this study gives a strong data support ,that patients with moderate COPD can improve their pulmonary function & thoracic expansion using G.P.R method, which includes stretching and mobilization of thoracic muscles whereby there is an increase in extensibility, flexibility and strength of major thoracic musculature for easy and better pulmonary function.
CONCLUSION
The study showed that there is a significant difference in improvement of FEV1/FVC ratio and thoracic expansion in Group –B who underwent Global postural re- education method than Group-A, who underwent conventional pulmonary rehabilitation.
Thus GPR method is better intervention in the improvement of pulmonary function, thoracic expansion in patients with moderate chronic obstructive pulmonary disease.
Limitations: This study was done during late summer when allergic stimuli were minimal. Certain factors such as nutritional, psychological factors could not be controlled. Drug profile was followed as such by pulmonologist.
Recommendations: Study can be done using large samples. Study can be done with mild or severe COPD patients. Study can be carried out for other respiratory diseases like bronchiectasis.
Ethical Clearance: An initial application was addressed to Research Ethics Committee, K G College of Physiotherapy and approval received for conduct of this study.
Conflict of interest: There was no conflict of interest on conduct of this study.
Fund for the study: It was aself financed study.
REFERENCES
- Hurd S. (2000).The Impact of C.O.P.D in lung health worldwide; Epidemiology and incidence;Chest; 117; 15-45.
- Coutinho EL, Gomes AR. (2004). The effect of passive lengthening on immobilized soleus muscle fibre morphology. Brazilian journal of respiratory medicine; 37(12); 1853-61.
- R.H.Green et al., (2001). A randomized controlled trial of four weeks versus seven weeks of pulmonary rehabilitation in chronic obstructive pulmonary disease. Thoracic journal of international medicine; 56; 1-48.
- Belman M J. (1996).Bronchodilator therapy reduces hyperinflation during exercise in patients with chronic obstructive pulmonary disease. American respiratory critical care medicine; 153; 967-975.
- Shah SB, et.al, (2001).Regulation of Sarcomere number maintained after immobilization in skeletal muscle. Journal Exp Biology; 204 (10); 1703-10.
- Surinder.k.et.al, (2006). Emergence of C.O.P.D as an epidemic in India. Indian journal Med.; Res December; 619-630.
- Julie A. Ekstrum, (2009). Effects of a Thoracic expansion and Respiratory Exercise Program on Pulmonary Function and Functional Capacity in Older Adults. Physical & Occupational Therapy in geriatrics; Vol. 27; No. 4; Pages 310-327.
- James. I. Cynthia cane (1995). Pulmonary rehabilitation-effects of exercise capacity in elderly patients with chronic obstructive pulmonary disease. Chest journal; Vol 107; pp730-34.
- Donarwee, (2008). Clinical effects of chest wall-stretching Exercise on expired tidal volume, dyspnea and chest mobility in patients with chronic obstructive pulmonary disease; A single case study.
- Combach. W. (1999). Long-term effects of pulmonary rehabilitation in patient chronic obstructive pulmonary disease: Arch of phy med and rehab; 80(1); pp-103-111.
- Blanco C, Cabezas M, et.al. (2005). Exercise interventions for the management ankylosing spondylitis: a randomized controlled trial. American Journal of Physical Medicine and rehabilitation; 84(6); 407-19.
- Elaine Pauline (2003). Physical exercises programme targeted to increase thoracic expansion in patients with obstructive lung disease. Pulmonology; Vol 29 (5).
- Gossmann MR, et al,. (1982). Review of length related changes in muscle. Experimental evidence and clinical applications. Physical therapy; 62(12); 1799-808.
- Derenne J P. (1978). The respiratory muscles: function and control, and patho-physiology. Am Rev Respiratory disease; 118(1); 119-33.
- Durmus .D, (2009). Effects of exercise interventions on pulmonary functions in the patients with ankylosing spondylitis . Joint bone spine; 76(2); 150-5.
- Souchard PE. (1987). Global postural reeducation: Method; 91-104.
- Montaldo BC. (2000).Breathing control. Chest; 117; 206-20.
- Kakisakhi (1999). Preliminary reports on effect if respiratory muscle stretches on thoracic mobility in individuals with obstructive lung disease. Respiratory care; (44); 409-14.
Citation:
| Ishwarya Vardhini C, Dennis Robinson, Jibi Paul (2019). A study to analyze the effects of global postural re-education method on pulmonary function and thoracic expansion in individuals with moderate chronic obstructive pulmonary disease , ijmaes, 5(3), 594-603. |