

Lisnaini
Corresponding Author:
Physiotherapy Program, Faculty of Vocational Studies, Universitas Kristen Indonesia, Jakarta
Mail id: lisnaini@uki.ac.id
| ABSTRACT |
Background: Diastasis Recti Abdominis (DRA) is a stretching and widening of the linea-alba which is a connective tissue that stretches in the middle of the abdomen that occurs in the second trimester to the third trimester and will continue until after delivery. Usually it cause complaints such as abdominal muscle weakness, lower back pain and posture disorders. Efforts that can be made to reduce the dilation of the postnatal linea-alba are by therapeutic exercise or physical exercise on the abdominal muscles. This study will focus on plank exercise was conducted to determine its effect on reducing the distance of the DRA below umbilicus.
Method: This research is a quantitative analysis with a quasi-experimental design that uses a two-group approach where the treatment was only given to one group and the other group only as a control.
Result: There was a reduction in the width of the diastasis rectus abdominis below the umbilicus by (67.7%) or as many as 42 people who did plank exercise while in the control group only (75.8%) or as many as 47 people who experienced a reduction in the width of the DRA lower umbilicus.
Conclusion: There is an effect of plank exercise on changes in the distance of the DRA below umbilicus and there is a relationship between plank exercise and a reduction in the width of the DRA below umbilicus in postpartum women.
Keywords: Diastasis Recti Abdominis; Postpartum; Plank exercise; Physiotherapy
| Received on 4thFebruary 2022, Revised on 19thFebruary 2022, Accepted on 26thFebruary 2022, DOI:10.36678/IJMAES.2022.V08I01.007 |
INTRODUCTION
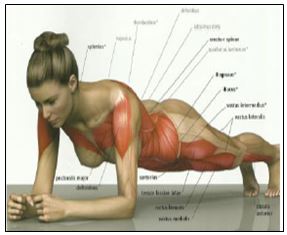
Diastasis Recti Abdominis (DRA) is stretching and widening of the linea alba, which is the connective tissue that runs down the middle of the abdomen and connects major abdominal muscles such as external obliques, internal obliques, transversus abdominis, and rectus abdominis1. Some researcher also stated that this condition usually happens when entering the second trimester and will become clearer in the third trimester and will continue after childbirth (postpartum)2,3.
Diastasis Recti Abdominis will widen due to frequent pregnancies. It also occurs because during pregnancy there is an increase in body weight and an increase in the hormonal levels of relaxin, progesterone, and estrogen from the connective tissue which causes mechanical pressure on the abdominal wall by the growing fetus so that the connective tissue becomes soft and the linea alba becomes tenuous4.
Almost 100% of pregnant women experience DRA5,6. Approximately 50% of nulliparous women experienced DRA and in women who undergo abdominal surgery and in postmenopausal patients7.Factors causing DRA are found in women who do excessive abdominal exercises especially in the first trimester, women who like to use hormone therapy, women who perform repeated operations on their abdomen, women with multiple pregnancies, large babies, and caesarean sections8. Ambarwati and Candido also stated that age and multiparity can be risk factors for rectus abdominis diastasis in women9,10.
Several studies have stated that the general impacts of DRA are the weakness of the abdominal muscles, urinary incontinence, decreased elasticity of the abdominal wall, functional and cosmetic disorders, low back pain5,6,9. Furthermore, about 52% of patients with urogynecological disorders stated that they had DRA and about 66% had complaints of pelvic floor muscle weakness such as stress urinary incontinence, stool incontinence and/or pelvic organ prolapse7.
Efforts that can be made to reduce the dilation of the postnatal linea alba are by therapeutic exercise or physical exercise on the abdominal muscles4. Previous research by Gitta et al. (2016) which stated that static contraction exercises in the abdominal muscles have been shown to reduce the DRA distance11. Research by Acharry & Kutty (2015) also stated that to prevent and reduce the DRA, physical therapy can be carried out after childbirth12. Another research by Wijayanti, (2016) proved that abdominal circumference can be reduced by strengthening abdominal muscles, sit-ups, postpartum exercise, physiotherapy, and plank exercise13.
Plank exercise is a type of static contraction exercise that is isometric exercise, which is muscle contraction exercises against resistance without causing changes in muscle length and joint motion14. This exercise can activate neuro-adaptive and proprioceptor mechanisms through altered sensory input to muscles. Lee et al.,stated that muscle activity in plank exercise is related to posture and muscle position exercises and has been proven to strengthen core muscles (especially transverse abdominis)15.
Based on all previous evidences obtained that exercise and physical exercise of the abdominal muscles can prevent and reduce postnatal women’s problems such as reducing abdominal circumference and increasing abdominal muscle strength. This study willfocus on plank exercise was conducted to determine its effect on reducing the distance of the DRA below umbilicus.
METHODS
This research is a quantitative analysis with a quasi-experimental design that uses a two-group approach where the treatment was only given to one group and the other group only as a control16. Meanwhile, the research design used pre and post-test design and how to take samples using a purposive sampling method.This study aims to determine the effect of plank exercise on DRAin women postpartum. Before and after being given treatment, the sample was measured for the length of the uterus by palpation and using a measuring device,calipers. The number of postpartum women who participated in this study was 124 people and was divided equally into 62 people in each group.
This research was conducted in the working area of the Makassar District Health Center, East Jakarta, and was carried out from April 2019 to June 2019. Plank Exercise intervention is carried out 3 times a week for 6 weeks.
The criteria set for the research sample are as follows:
Inclusion criteria:
- All postpartum women at the Makassar District Health Center, East Jakarta and the Kebon Pala Village Health Center, East Jakarta
- Postpartum woman with minimum 2 hours after delivery
- Postpartum women with DRA (>2.5 cm)
- Postpartum women with a disease history of vaginal delivery
- Willing to follow an exercise program regularly.
- Willing to not do activities that are suspected of affectingDRA, such as participating in other gymnastics activities outside the given program.
- Willing to be a sample and sign informed consent.
Exclusion Criteria:
- Postpartum women who refused to participate in this study
- Postpartum women who have participated in postpartum gymnastics and other physical activities
- Postpartum women who are having heart problems, respiratory problems including excessive coughing or sneezing
- Postpartum women with pelvic or abdominal surgery (except for cesarean section), neurological disease, bowel or bladder trauma
- Depressed postpartum woman
Measurement of DRA:
Measurement by palpation of the fingers and calipers DRA measurements were carried out before and after plank exercise. According to Bursch, Mantle et al. and Rett et al. (2009), the palpation measurement technique meets the criteria of reliability and ease to use. The measurement can be done by placing a finger palpation between the medial border of the right and left rectus abdominis muscles, which is parallel to the linea alba3,17,18.
The size of DRA is determined by the number of fingers that enter between the two gaps in the abdominal wall that are the muscles above and below the umbilicus when the individual performs the movement placing her chin on her chest. Clinically, this palpation technique is simple.

1.Measurement procedure by palpation is carried out as follows:
- Make the subject lying flat on her back without a pillow under her head.
- Place the fingertips of one hand on the midline of the abdomen with the tip of the index finger just below the umbilicus and the other finger lined longitudinally downward toward the symphysis pubis.
- Ask the subject to raise her head to rest her chin on her chest in the area between her breasts. Make sure not to press her hands against the bed or grip the mat to help her, as this prevents the use of the abdominal muscles.
- As the subject attempts to rest her chin between her breasts, gently press your fingertips close to her abdomen. You will feel the abdominal muscles like two rubber bandages approaching the midline from either side.
- Measure the gap between them with calipers when the muscles are contracted.
- Note the distance between the two slits
- When lowering the head, the abdominal muscles move further apart and are less distinguishable when the muscles are relaxed. Your fingertips will follow the rectus muscle apart to the lateral side of each abdomen.
- Measure the distance between the two rectus muscles when they are relaxed.
- Note the measurement results
2. Measurement using calipers
Measurement procedure the rectal distance was measured using a caliper technique, the participant was in a lying position with a pillow under the head and feet resting on the base and arms by the side of the body. The desired measurement location is marked 4.5 cm above the midpoint of the umbilicus and 4.5 cm below the midpoint of the umbilicus. Each participant raises their head until the spine of the scapula is off the table surface.
Participants were asked to maintain this position while the examiner palpated the medial border of the right & left abdominis abdominal muscles at the marked area. Measuring the inside of the jaws of a digital nylon caliper, positioned at the location of the palpated finger, perpendicular to the direction of the muscle and adjusted for the width of the perceived intra-rectal distance. Three measurements were taken for each assessment and then recorded. Participants are allowed to rest between measurements and are also allowed to rest if they feel tired 21.

Intervention Group
In the treatment group, interventions were given in the form of plank exercise.Plank exercise is an isometric type of exercise, which is a type of static muscle contraction exercise against resistance without any change in muscle length or not followed by joint movement14. This exercise begins by extending the legs while supporting the upper body with the arms. Bend elbow position, hold abdominal and gluteal muscles.
This exercise is done 3 times a week for 6 weeks with 3 repetitions of each exercise. The prone plank exercise is carried out by holding it for 30 seconds for each movement then resting for 15 seconds and then repeating it 20.
Control Group
In the control group, the research sample was given an education program in the form of counseling on the importance of exercise to restore the health of postpartum women with DRA conditions. Based on research, regular exercise can also improve the DRA4.
RESULTS AND DISCUSSION
Following is the distribution of Plank Exercisevariables and the control group
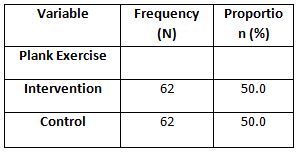
Based on table 1, each postpartum woman performs Plank Exercise that the intervention group also included 62 people (50%) and the control group with 62 people (50%).
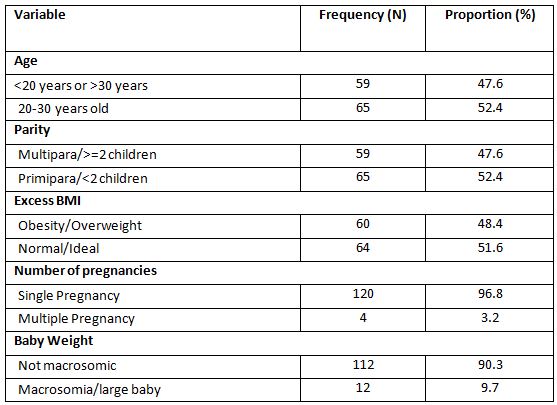
Based on table 2, the number of postpartum women aged < 20 years or > 30 years was 59 people (47.6%), multiparous status was 59 people (47.6%), had Obesity/Overweight BMI which was 60 people (48.4%), history of singleton pregnancy namely 120 people (96.8%), and the weight of newborns was normal (not macrosomic) that was 112 people (90.3%).
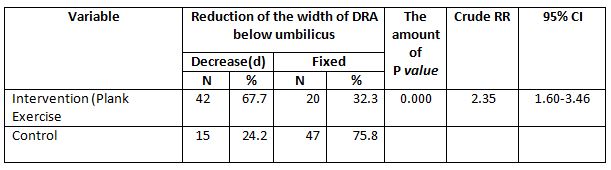
Relationship between Independent and Confounding Variables on Reduction of the width of the DRA below umbilicus)
While most of the postpartum women who do not do plank exercise did not experience a reduction in the width of the DRA below umbilicus (fixed) was 47 people (75.8%). Chi Square test results stated that there is a relationship between plank exercise with a reduction in the width of the DRA below umbilicus (p value <0.05).
Postpartum women who did Plank Exercise had a 2.3 times chance of experiencing a reduction in the width of the DRA below umbilicus compared to those who did not do it (p value =0.000; cRR=2.35;95%CI= 1.60-3.46).
Based on Table 4, the results of the cross-tabulation show that most of the postpartum women aged < 20 years or >30 years did not experience a reduction in the width of the DRA below umbilicus (fixed) was 31 people (52.5%). While those aged 20-30 years most did not experience a reduction in the width of the DRA below umbilicus (fixed) was 36 people (55.4%). Chi Square test results showed that there was no relationship between age and a reduction in the width of the DRA below umbilicus (p value> 0.05).
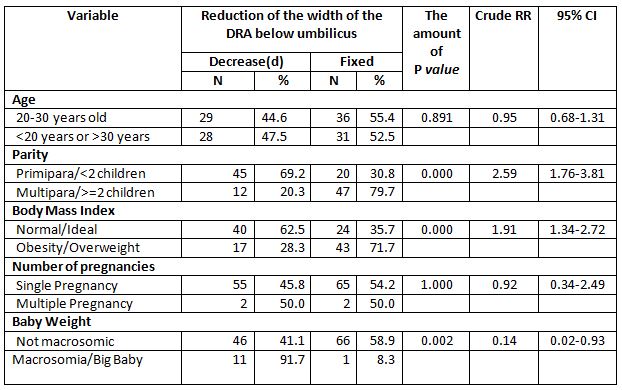
The results of cross tabulation showed that most of the postpartum women with multiparous status did not experience a reduction in the width of the DRA below umbilicus (fixed) was 47 people (79.7%). While most of the primipara experienced a reduction in the width of the DRA below umbilicus was 45 people (69.2%). Chi Square test results stated that there is a relationship between plank exercise with a reduction in the width of the DRA below umbilicus (p value <0.05). Primipara postpartum women were 2.6 times more likely to experience a reduction in the width of the DRA below umbilicus than multiparous women (p value =0.000; cRR=2.59;95%CI= 1.76-3.81).
The results of the cross tabulation showed that the postpartum women who were obese/overweight mostly did not experience a reduction in the width of the DRA below umbilicus (fixed) was 43 people (71.7%). Meanwhile, postpartum women with normal/ideal BMI experienced a reduction in the width of the DRA below umbilicus was 40 people (62.5%). Chi Square test results showed that there was a relationship between excess BMI and a reduction in the width of the DRA below umbilicus (p value <0.05). Postpartum women with normal/ideal BMI were 1.9 times more likely to experience a reduction in the width of the DRA below umbilicus compared to obesity/overweight (p value=0.000; cRR=1.91;95%CI=1.34-2.72).
The results of cross tabulation showed that postpartum women with multiple pregnancies 50% experienced a reduction in the width of the DRA below the umbilicus. While postpartum women with singleton pregnancies mostly did not experience a reduction in the width of the DRA below the umbilicus (fixed) was 65 people (54.2%). Fisher Exact test results showed that there was no relationship between multiple pregnancies with a reduction in the width of the DRA below umbilicus (p value> 0.05).
The results of cross tabulation showed that postpartum women who gave birth to babies weighing 4000 grams mostly experienced a reduction in the width of the DRA below the umbilicus was 11 people (91.7%). Meanwhile, postpartum women with babies weighing <4000 grams mostly did not experience a reduction in the width of the DRA below umbilicus (fixed) was 66 people (58.9%). Chi Square test results showed that there was a relationship between large baby weight and a reduction in the width of the DRA below umbilicus (p value <0.05). Postpartum women with not macrosomic babies were 0.1 times more likely to experience a reduction in the width of the DRA below umbilicus compared to women with macrosomic babies (p value=0.002; CRR=0.14;95%CI=0.02-0.93).
The results of this study are in line with research by Fitriahadi 21. With a quasi-experimental research model and similar types of interventions. The results of the study stated that most of the decrease in DRA occurred quickly in the treatment group (plank exercise) by 10 (66.65), while a slower decline in DRA occurred in the untreated group (control group) by 9 (60%), supported by bivariate analysis with p value = 0.003, this proves that there was an effect on strengthening the rectus abdominis muscle to reduce the DRA distance in postpartum women.
The results of the study are in line with previous research that there was an effect of sit-up exercise with prone plank exercise on decreasing abdominal circumference in adolescent girls13. Other research also stated that exercise will have an effect after being done for 6 weeks, for example, weight training can increase muscle strength by 20.1% within those weeks22. In general, previous research by Khandale & Hande also stated that abdominal muscle training can reduce DRA in early postpartum women and can prevent complications due to DRA23.
This research still has some limitations. This research method is still very simple and needs to be improved for the better in future research. The examination is also carried out in a simple manner, the use of other, more sophisticated examination tools is needed in future research. Likewise, this study only evaluates short-term effects, then, long-term research to determine long-term effects also needs to be done. The use of the results of this study must be responsible to avoid misunderstanding.
CONCLUSION
Based on data analysis, it was found that there was a reduction in the width of the DRA below umbilicus in postpartum women with treatment of 42 people (67.7%) while in the control group only 15 people (24.2%). Thus, it can be concluded thatthere is an effect of plank exercise on changes in the distance of the DRA below umbilicus and there is a relationship between plank exercise and a reduction in the width of the DRA below umbilicus in postpartum women.
Recommendations: As a recommendation from this study, physiotherapists would be able to advise postpartum women to do plank exercise in reducing various postnatal complaints and increasing quality of life both in the community and at home.
Ethical Clearance: This research was approved by the East Jakarta Health Service Center with reference number 1950/1.772.2.
Acknowledgements: We would like to thank the postpartum women in Makassar Health Center, East Jakarta who are willing to participate in this research.
REFERENCE
1. Lee D, Lee L, McLaughlin L. Stability, continence and breathing: The role of fascia following pregnancy and delivery. J Bodyw Mov Ther. 2008;12(4); 333-348.
2. Estiani M, Aisyah A. Faktor-Faktor Yang Berhubungan Dengan Kejadian Diastasis Rekti Abdominis Pada Ibu Post Partum Di Wilayah Kerja Uptd Puskesmas Sukaraya Baturaja. J Keperawatan Sriwij. 2018; 5(2); 24-31.
3. Rett MT, Braga MD, Bernardes NO, Andrade SC. Prevalence of diastasis of the rectus abdominis muscles immediately postpartum: Comparison between primiparae and multiparae. Brazilian J Phys Ther. 2009; 13(4) ;275-280.
4. Michalska A, Rokita W, Wolder D, Pogorzelska J, Kaczmarczyk K. Diastasis recti abdominis – A review of treatment methods. Ginekol Pol. 2018; 89(2):97-101.
5. Mota P, Pascoal AG, Carita AI, Bø K. Normal width of the inter-recti distance in pregnant and postpartum primiparous women. Musculoskelet Sci Pract. 2018;35; 34-37.
6. Walton LM, Costa A, LaVanture D, McIlrath S, Stebbins B. The effects of a 6 week dynamic core stability plank exercise program compared to a traditional supine core stability strengthening program on diastasis recti abdominis closure, pain, oswestry disability index (ODI) and pelvic floor disability index score. Phys Ther Rehabil. 2016;3(1); 3.
7. Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J. 2007;18(3); 321-328.
8. Aswini D, Srihari SK. An Overview of the Studies on Diastasis Recti Abdominis in Postpartum Women. J Gynecol Womens Heal. 2019; 14(5).
9. Ambarwati ER. Asuhan Kebidanan Nifas. Nuha Medika; 2010.
10. Candido G. LT. JPA. Risk factors for diastatis of the recti abdominis. J Assoc Chart Physiother Women’s Heal. 2005;97(January 2005); 49-54.
11. Gitta S, Magyar Z, Tardi P, et al. How to Treat Diastasis Recti Abdominis with Physical Therapy: A Case Report. J Dis. 2016;3(2); 16-20.
12. Acharry N, Kutty RK. Abdominal Exercise With Bracing, a Therapeutic Efficacy in Reducing Diastasis-Recti Among Postpartal Females. Int J Physiother Res. 2015; 3(2); 999-1005.
13. Wijayanti D. Perbedaan Pengaruh Sit-up Exercise Dan Prone Plank Exercise Terhadap Penurunan Lingkar Perut Remaja Putri. Publ Manuscript, Univ Aisyiyah Yogyakarta. Published online 2016; 1-16.
14. Schoenfeld BJ, Contreras BM. The long-lever posterior-tilt plank. Strength Cond J. 2013; 35(3):98-99.
15. Lee J, Jeong K, Lee H, et al. Comparison of three different surface plank exercises on core muscle activity. Phys Ther Rehabil Sci. 2016;5(1); 29-33.
16. Sugiyono. Metode Penelitian Pendidikan Pendekatan Kuantitatif, Kualitatif Dan R&D. Alfabeta; 2013.
17. Bursch SG. Interrater reliability of diastasis recti abdominis measurement. Phys Ther. 1987;67(7); 1077-1079.
18. Mantle J, Haslam J, Barton S. Physiotherapy in Obstetrics and Gynaecology. Elsevier Ltd; 2004.
19. Chiarello CM, McAuley JA. Concurrent validity of calipers and ultrasound imaging to measure interrecti distance. J Orthop Sports Phys Ther. 2013;43(7); 495-503.
20. Bennett VR, Brown LK. Myles Textbook for Midwives. Churchill Livingstone; 1999.
21. Fitriahadi E. Pengaruh Penguatan Otot Rectus Abdominis Terhadap Penurunan Tfu Pada Ibu Postpartum Pervaginam Di Bpm Kabupaten Sleman. J Kebidanan. 2019; 8(1); 61.
22. Sudarsono S. Penyusunan Program Pelatihan Berbeban Untuk Meningkatkan Kekuatan. J Ilm SPIRIT. 2015;12(1); 31-43.
23. Khandale SR, Hande D. Effects of Abdominal Exercises on Reduction of Diastasis Recti in Postnatal Women. Int J Heal Sci Res. 2016; 6(6); 182. www.ijhsr.org
| Citation: Lisnaini. Effect of plank exercise on diastasis recti abdominis lower umbilicus in postpartum women, International Journal of Medical and Exercise Science, March 2022; 8(1): 1219-1227. |
Leave a Reply