

Manoj Abraham. M1, Soumya Murali2
Author:
1Principal, KG college of Physiotherapy (The Tamil Nadu Dr. M.G.R. Medical University), Thudiyalur Road, Saravanampatti, Coimbatore, Tamilnadu, India, Email id: manojpt3@gmail.com
Corresponding Author:
2BPT Internee, KG college of Physiotherapy (The Tamil Nadu Dr. M.G.R. Medical University), Thudiyalur Road, Saravanampatti, Coimbatore, Tamilnadu, India, Email id: soumyamurali2818@gmail.com
ABSTRACT
Background: Upper crossed syndrome occurs due to muscular imbalance created in opposite muscle groups developing due to postural disturbances. It is presented with the simultaneous tightening of postural muscles and weakening of non-postural muscles in the upper body resulting in limited mobility. The purpose of the study is to determine the prevalence of upper crossed syndrome among software professionals.
Methods: A randomized sampling of 106 software professionals was conducted based on inclusion and exclusion criteria. The research was a cross-sectional study where software professionals of age group 20-40 years having a daily working schedule of minimum of 3 hours and a maximum of 18 hours on computers were included. A self-designed questionnaire and Neck Disability Index were circulated among participants and were assessed by performing special tests.
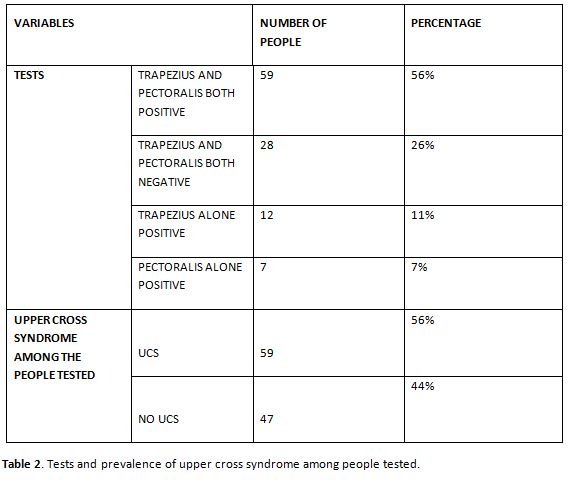
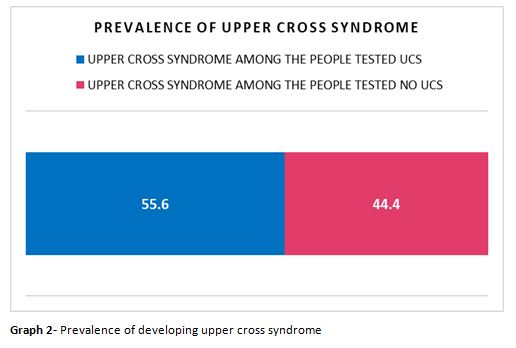
Results: The prevalence of upper crossed syndrome among the software professionals is 55.6%. There is a positive linear relationship between the development of the upper crossed syndrome and the functional disability among the people and in the Neck Disability Index and the hours of working in front of computer.
Conclusion: This study illustrates that there is a significant prevalence of upper crossed syndrome among software professionals. Neck pain and functional limitation were presented as the main symptom that is in the verge of occurrence.
Keywords: Upper crossed syndrome, musculoskeletal imbalance, neck disability index.
Received on 29th July 2021, Revised on 10th August 2021, Accepted on 26th August 2021, DOI:10.36678/IJMAES.2021.V07I03.004
INTRODUCTION
India has been the vanguard in the cyber world with the development of information techno-logy. Approximately 6 computers per 1000 population and about 18 million personal computers are prevalent in our country. This number is increasing day by day. The booming of the information technology industry in India has led to an increase in the use of computer devices as well as marked the start of a new genre of occupational health problems among software professionals1. It has led to various musculoskeletal discomforts2. The mushroom-ming of the Visual Display Units (VDU) or the Visual Display Terminals (VDT) in the modern office settings has led to the various occupational health problems and musculo-skeletal ailments associated with it3. With the association of improper posture, excessive muscular tension, and limited mobility results4. The excess time on work demands results in a significant increase in pain, functional limita-tion and fatigue5.
The physiological response from the work has been termed as “workstyle”. Workstyle has been recognized as a coupling factor for the muscular imbalances creating pain and functional limitation dueto the ergonomic factors inthe computer users6. Among the musculoskeletal complaints, the neck was the common site to be affected because of the static posture during work hours in front of the computer7.
While working in a sitting posture for a prolo- nged time, they tend to adopt a forward head posture shifting the head forward to the spinal central line. This is because they find it difficult to maintain the normal posture of the spine during the prolonged work hours of sitting8. For every one inch of forward head posture, there is an increase of additional 10 pounds of weight of head on the spine. Where the poor sitting may result in forward head posture and rounded shoulders due to altered body kinematics9. This forward head posture results in mechanical stress on the neck and cause smuscular imbalances10 where onegroup of muscles gets tightened and the other group gets weakened and inhibited11.
This leads to the weakening of middle, lower trapezius, rhomboid scrossing ventrally with the weakness of significant cervical flexors. Simultaneously, the tightening and over active upper trapezius, levator scapulae crossing dorsally with the tightness of pectoralis major and minor also occur12. This may also cause rounded shoulder, and abnormal postures of shoulder blades. Janda defined this phenom- enon as Upper Crossed Syndrome (UCS)13. Dr. Vladimir Janda coinedthis syndromeas Upper Crossed because when the weakened and tightened muscles form a cross when they are connected in the upper body14.
These muscular imbalances created in upper crossed syndrome in opposite muscle groups develop postural disturbances. This would res- ult in a reduction of the quality of the glenohu- meral joint. This is because the glenoid cavity will become more vertical because of the serratus anterior weakness creating the scapulae for winging and turning15. Sitting with the posture of forward head position creates upper cervical region extension and lower cervical region flexion which will in turn, reduce the muscle fiber length. This will eventually develop extensor torque around the upper cervical joints which will later lead to musculoskeletal imbalances and abnormalities like reduced scapular upward rotation, incre- ased internal rotation, anterior tilt which will eventually make them more difficult to maintain their erect posture of sitting16. This winging, elevated, and abducted scapula creates scapular dyskinesia there by which creates inrounding of shoulders.
Nearly three-fourths of the software profess- ionals were identified with computer- related health problems and musculoskeletal ailments. This is almost a significant proportion of the population of software professionals. This den- otes a need to emphasize a field of concern among the software professionals, their well being, and occupational health. Hence regular health check-ups and ergonomic advice being sensitized regarding the importance of their wellbeing and proper working conditions17.
METHODOLOGY
This was a cross-sectional study that was conducted in the Physiotherapy Outpatient Department, KGiSL Campus, Saravanampatti, Coimbatore. This study included 106 particip- ants who were selected by a simple random- ized sampling method. The study duration was three months. Epistat info was used for sample size calculation.
The objectives of the study were; to identify the occurrence of upper crossed syndrome among software professionals; to correlate the upper crossed syndrome with the functional disability of the individuals and also to correlate the upper crossed syndrome with the working hours infront of computer among software professionals.
Procedure: A written consent is obtained from every individual who signed up for the study. Before the study, a brief instruction was given regarding the research. Individuals selected for the study were instructed and asked to assemble in the K.G Outpatient Department in Coimbatore. Aself-designed questionnaire was distributed, the first section of which question- naire was focused on demographic details (name, age, gender, years of working) and the second section included social factors (personal and past history of any illness or treatment), the third section included the occ-urrence of neck pain(onset, duration and past treatment ), the fourth section consisted of other factors (history of working details and confirmatory tests) after the filling up of ques-tionnaire the subjects were also given the Neck Disability Index (NDI).
Neck disability index (NDI): It is a self-reported condition-specific questionnaire that includes 10 items- pain intensity, personal care, lifting, reading, headache, concentration, work, driving, sleeping, recreation). This questio- nnaire emphasizes how neck pain affects the ability to manage the activities of daily life (ADL).
The questionnaire was validated by 3 senior physiotherapists who are involved in occupational health research. After completion of filling the data, Trapezius and pectoralis tests are performed. The collected data were noted and taken for analysis. After the compl- etion of the procedure, thank you note accom- panied with ergonomic advice and a postural awareness pamphlet was given to subjects.
Inclusion criteria: Age between 20-40 years18, Software professionals with a computer-related work experience of minimum of 6 months18, with duration of working hours taken into consideration whichis fixed as at least 3 hours a day or 15 hours per week1.
Exclusion criteria: previous history of any surgery/underlying pathology/inflammatory di- seases to cervical spine, known history of fractures of cervical spine or tumors18,19.
RESULTS
This study showed that a significant proportion of software professionals in the present study reported that they experience muscular disco-mforts. This may be due to various factors such as the impact of the prolonged working hours in poor posture, involvement of multiple joints in computing tasks, adopting biomechanical and anatomical alignment of body motions of high physiologic cost leading to muscular imbalances gradually.
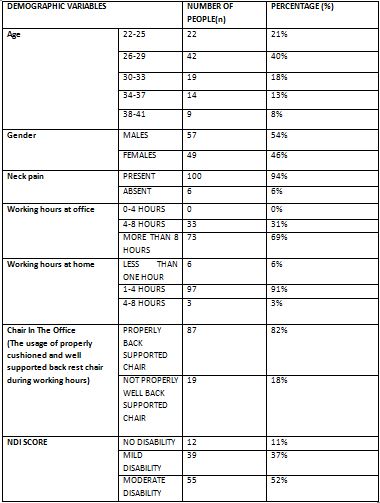
Most of the subjects spent a prolonged time in the office as their working hours showed that 31% of the population worked in front of the computer for 4-8hours and 69% of them had more than 8 hours of working on the computer with a static posture. Due to this static posture, they develop symptoms of neck pain. Out of 54% males and 46% females selected rando- mly, 94% of the population reported neck pain and 6% had no neck pain. 30(28%) of them experienced pain for less than one year, 40 (38%) mentioned that they are experiencing pain for one to two years and 36(34%) population had pain for more than 2 years. It was also discovered that only 82% of the population had proper back-supported well-cushioned chairs and the remaining 18% had no properly back supported chair in the office which can be a potential ergonomic risk for the yielding of symptoms as they work for prolonged hours.
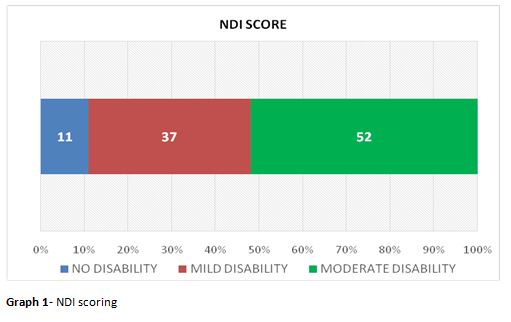
Neck Disability Index values revealed that 11% of them had 0-8% of scoring stating no disability, 37% of them had mild disability scoring 10-28%, 52% of them scored 30-48% had moderate disability. None of the popula- tion had severe or complete disability. Further from the study, it was found that the symptoms and muscular discomforts were most debilitating causing a reduction in Activ- ities of Daily Living(ADL).
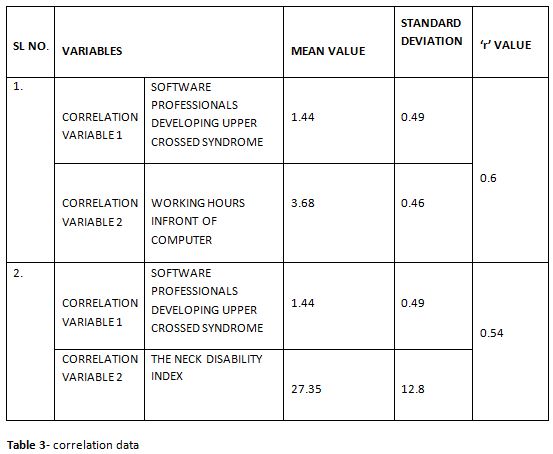
The mean value of the software professionals who are on the verge of developing upper crossed syndrome is 1.44±0.49 subjects and the mean value of their working hours is 3.68±0.46 hours. The value of ‘’r’’ value correlating them is 0.60. This is a moderate uphill (positive) linear relationship between the development of the upper crossed syndrome and the hours of working among software professionals in front of the computer.
The mean value of the software professionals who are on the verge of developing upper crossed syndrome is 1.44±0.49 subjects and the mean value of their functional disability in Neck Disability Index scale is 27.35±12.8.The value of “r” correlating them is 0.54. This is a moderate uphill (positive) linear relationship between the development of the upper crossed syndrome and the functional disability among the people on the neck disability index.
DISCUSSION
The study has focused on the prevalence of upper crossed syndrome among software professionals. Christensen Ketal, in 2015 evide- ntly proposed upper crosss yndrome appears to be a simple muscular imbalance but it may impart huge stress on the economy of the country via resulting in functional disability due to neckpain20.
As derived from this study, work organization plays an important role, especially when ergonomic measures are largely implemented. A study also has reported that the individuals developing upper cross syndrome were some how associated with bad postureor indulge in any activity that makes them adopt a posture of high physiologic cost thereby leading to a muscular imbalance that will yield upper cross syndrome21. Morrisetal, Stated that the correlation between upper cross syndrome and poor posture is relevant and found the subjects suffering from the upper cross syndrome were mostly because of poor posture or due to any those activity that makes them adopt bad posture developing a muscular imbalance that will yield upper cross syndrome22.
As Kwonetal, in a study in 2015 suggested that If proper steps are not taken at the initial moment when identified with neck pain with functional disability this may become an endemic not only in the working population but also in the people who tend to adopt a poor posture and least bothered regarding their posture, it is suggested that there should be a pace in the blow to generate postural awareness in people of all ages and most predominantly the risk groups who are in the verge of the occurrence of upper crossed syndrome gradually23.
After review and knowing that neck pain is the main symptom initiated, Neck Disability Index was used as the outcome measure used to assess the impact of neck pain on activities of daily living (ADLs). Most of them had neck disability associated with muscular imbalances. On studying musculoskeletal symptoms of the upper extremities and the neck with symptom-predicting factors at visual display terminal (VDT) workstations, preventive measures should be focused on neck and shoulder disorders. So, for preventive aspect this study also states that ergonomic interventions sho-uld be implemented.
CONCLUSION
It is concluded that most of the software professionals were having muscular imbalances yielding upper crossed syndrome and experie- nced the muscular ailment symptoms of neck pain leading to functional disability. The prevalence of neck pain to be 94.3% and the verge of developing upper crossed syndrome to be found as 55.6% among the software professionals. They were exposed to the risk of adopting poor postures due to extended periods of working hours in a static posture. This study provides knowledge that ergonomic advice to be educated and postural awareness should be introduced and proper biomechanics to be utilized during work hours to enable the work efficiently and comfortably thus improving productivity.
Limitations And Recommendation: This study does not focus on any treatment to the participants as the present study only consisted of ergonomic advice and was done within a limited geographical location there by decrea-sing generalizability. No diagnostic tests other than trapezius and pectoralis tests are included. Future studies could evaluate the association between the occurrence of Work-Related Musculoskeletal disorders and various psychosocial factors such as high stress, low control among the Software professionals. Radiographic diagnostic procedures can be done for the findings. A similar study can be conducted on a wider age group to find out theage impact on the development of the upper crossed syndrome. Treatment protocols can be given for the selected population as the present study consisted of ergonomic advice only.
Ethical Approval: Ethical clearance has been obtained from the K.G College of Physiotherapy Ethical Committee.
Conflicts Of Interest: No conflict of interest to conduct and publish this article was reported throughout the study.
Fund For The Study: This study is self-funded.
Acknowledgement: The authors would like to express sincere gratitude and special thanks to all the participants who took part in the research.
REFERENCES
- Sharma, A. K., Khera, S., &Khandekar, J. (2006). Computer relatedhealthproblems among information technology professionals in Delhi. Indian journal of community medicine, 31(1); 36.
- Talwar, R., Kapoor, R., Puri, K., Bansal, K., & Singh, S. (2009). A study of visual and musculoskeletal health disorders among computer professionals in NCR Delhi. Indian journal of community medicine: official publication of Indian Association of Preventive & Social Medicine, 34(4); 326.
- Singh, S., & Wadhwa, J. (2006). Impact of computer workstation design on health of the users. Journal of Human Ecology, 20(3); 165-170.
- Moore, M. K. (2004). Upper crossed syndrome and its relationship to cervico-genic headache. Journal of manipulative and physiological therapeu- tics, 27(6), 414-420.
- Lundberg, U. (2002). Psychophysiology of work: Stress, gender, endocrine response, and work‐related upper extremity disorders. American journal of industrial medicine, 41(5); 383-392.
- Feuerstein,M., Nicholas, R. A., Huang, G. D., Haufler, A. J., Pransky, G., & Robertson, M. (2005). Workstyle: development of a measure of response to work in those with upper extremity pain. Journal of occupational rehabilitation, 15(2); 87-104.
- Yu, I. T. S., & Wong, T. W. (1996). Musculoskeletal problems among VDU workers in a Hong Kong bank. Occupational medicine, 46(4); 275-280.
- Calliet, R. (1991). Mechanism of Pain in the Neck and From the Neck. Philadelphia: Neck and arm pain, 348-67.
- Janda, V. (1993). Muscle strength in relation to muscle length, pain and muscle imbalance. International Perspectives in Physical Therapy, 83-83.
- Waris, P. (1979). Occupational cervico brachial syndromes: a review. Scandinavian journal of work, environment & health, 3-14.
- Gu, S. Y., Hwangbo, G., & Lee, J. H. (2016). Relationship between position sense and reposition errors according to the degree of upper crossed syndrome. Journal of physical therapy science, 28(2); 438-441.
- Arora, D., &Veqar, Z. (2010). Correlation between endurance of deep cervical flexors and lower scapular stabilisers in computer users with chronic neck pain. British Journal of Sports Medicine, 44(Suppl 1); i11-i11.
- Janda, V. (1996). Rehabilitation of the spine. Baltimore: Williams & Wilins. 319-328.
- Umasankar Mohanty (2015), Manual therapy for upper crossed syndrome, J Nov el Physiotherapies, 5:4 http://dx.doi. org/10.4172/2165-7025.S1.001.
- Patterson, K., & Evans, O. M. (2000). Predictors of Neck and Shoulder Pain in Non-Secretarial Computer Users. Volume 26, Issue 3, September 2000; pp 357-365.
- Kang, J. H., et al (2012). The effect of the forward head posture on postural balance in long time computer-based worker. Annals of rehabilitation medicine, 36(1); 98.
- Blatter, B. M., &Bongers, P. M. (2002). Duration of computer use and mouse use in relation to musculoskeletal disorders of neck or upper limb. International Journal of Industrial Ergonomics, 30(4-5); 295-306.
- Kumar, S., Sambyal, S., &Vij, J. (2013). Analysis of disability and pain in Computer Professionals with Neck Pain. IOSR JNHS, 3; 6-9.
- Dahiya, J., & Ravindra, S. (2013). Effect of scapular position in computer professionals with neck pain. International Journal of Science and Research, 4(5); 2075-2080.
- Christensen, K. (2000). Manual muscle testing and postural imbalance. Dynamic Chiropratic, 18(24). November 15, 2000, Vol. 18, Issue 24.
- Mubeen I, Malik S, Akhtar W, Iqbal M, Asif M, Arshad A, Zia S,Khalid (2016). Prevalence of upper cross syndrome among the medical students of university of lahore. International journal of physio-therapy 3, no. 3 (2016); 381-384.
- 22. Morris,C.E.,Bonnefin, D., & Darville, C. (2015). The Torsional Upper Crossed Syndrome: A multi-planar update to Janda’s model, with a case series introduction of the mid-pectoral fascial lesion as an associated etiological factor. Journal of bodywork and movement therapies, 19(4); 681-689.
- 23. Kwon, J. W., Son, S. M., & Lee, N. K. (2015). Changes in upper-extremity muscle activities due to head position in subjects with a forward head posture and rounded shoulders. Journal of physical therapy science, 27(6); 1739-1742.
| Citation: Manoj Abraham. M1, Soumya Murali(2021). Prevalence of upper crossed syndrome among software professionals , ijmaes; 7 (3); 1061-1071 |
Leave a Reply