

Ishwarya vardhini. C1, Nelshiya Anni Ruby Aishwariya. H. P2
Author:
1Assistant professor, Faculty of physiotherapy, Dr.MGR Educational and research institute University, Velappanchavadi, Chennai, Tamilnadu, India
Corresponding Author:
2BPT Internee, Faculty of physiotherapy, Dr. MGR. Educational and research institute University, Velappanchavadi, Chennai, Tamilnadu, India, Email id: nelshiyaannirubyaishwariya@gmail.com
ABSTRACT
| Background of the study: Osteoarthritis (OA) knee is a commonest degenerative disorder, accompanied by pain, muscle weakness, and decreased ability to carry out activities of daily living. Strengthening of VMO is the exercise choice commonly used. Studies suggest that strengthening of hip abductor; can reduce the KOA-associated symptoms. Objective of this study was to find whether VMO in combination with hip abductor strengthening can improve the function and reduce pain in KOA. Materials and methods: 30 subjects with grade 1- KOA of both the genders belonging to age group from 45-60 years were chosen and subjected to VMO & hip abductor strengthening for a period of 12 weeks. Pre and Post exercise outcome scores were measured using VAS and WOMAC scale. Results: This study showed a substantial improvement of pain, stiffness and physical function in subjects who underwent VMO and hip abductor strengthening program. P-value on VAS and WOMAC scale was less than 0.0001 which was found significant. Conclusion: Hip abductor along with VMO strengthening is a better health interventionin subjects with Grade 1 Osteoarthritis knee .Thus hip muscle strengthening can serve a better intervention in slowing the progression of disease and reduction of symptoms in grade -1 KOA. |
Keywords: Grade-I-KOA; Hip Abductor Strengthening; Vastus Medialis Obliqus (VMO); WOMAC; VAS.
| Received on 28th January 2021, Revised on 18th February 2021, Accepted on 27th February 2021; DOI:10.36678/IJMAES.2021.V07I01.007 |
INTRODUCTION
Osteoarthritis of knee is the second most common chronic degenerative joint disease occurring among elderly. It leads to pain, muscle weakness especially quadriceps and disability which are the earliest clinical signs of OA knee1. OA knee is classified into 2 divisions. Primary OA knee is without any known reason (idiopathic) and ccurs in the elderly due to ageing process. Secondary OA knee is due to increased body mass index, family history, joint hyper mobility, repetitive strain to the knee, trauma, immobilization, neuropathic disorders 2.
The symptoms that halt the function include morning stiffness, reduced joint movement, crepitus and muscle atrophy 3. Diagnosis of knee osteoarthritis can be confirmed based on clinical and radiographical Findings .The American College of Rheumatology criteria , EULAR diagnostic criteria ,can be further used to diagnose KOA which includes presence of constant knee pain, morning stiffness reduce function, joint crepitus, restricted mobility and hypertrophy of bone. The available treatment options are non-pharmacological, pharmacological or surgery. Physical therapy is a least expensive intervention for OA knee which is recommended by the American college of Rheumatology and the European League against Rheumatism4.
Exercise is recommended as a first-line of conservative management option for osteoarthritis (OA). They can decrease pain status, improve joint mobility & functional ability. Quadriceps weakness is common among OA knee which in turn causes painful lower limb thereby making it a risk factor for development of OA. The function of quadriceps group of muscles, particularly VMO muscle has an important role in the stability of the patella-femoral joint 5. Reduction in activity of hip abductor muscle has been suggested as a contributing factor for the disease progression in knee osteoarthritis (OA).
Hip abductor strengthening can serve as an intervention to reduce knee joint loading in subjects with OA knee 6. Increased hip abduction moment magnitude is directly proportionate in reducing the progression of medial compartment OA knee7. Hip abductor weakness results in poor functional performance in subjects with OA. They are stabilizer of trunk & hip during walking, maintain the position of lower extremity and transmit the forces from the lower extremity to the pelvis8. Therefore inclusion of hip abductor exercises along with VMO can prove beneficial when designing a rehabilitation program for persons with knee OA.
METHODOLOGY
This was an Experimental study and the participants those attending the outpatient physiotherapy department in ACS medical college and hospital, Dr. MGR Educational and Research institute, Chennai India. The study duration was around 12 weeks. This study included 30 subjects with grade I Osteoarthritis knee (as per kellgrenn and Lawrence radio graphical grade(9) of both the genders in age-group between 45 and 60 years. The participants were selected by simple random sampling method. Subjects apart from grade 1 OA knee, non-cooperative subjects, those with balance, auditory, visual disorder, lower limb injury were excluded from the study.
The objective of this study was to find the effect of hip abductor and vastus medialis oblique muscle (VMO) strengthening exercises on Pain and Physical function were measured using VAS (Visual analog scale) and WOMAC (The Western Ontario and McMaster Universities Osteoarthritis Index).
Procedure: The subject’s pain & functional ability were documented using Visual Analogue Scale (VAS) in which the patient denotes pain level on the line between two endpoints. The distance between point of no pain and the marking measures the subject’s pain score(10). Then WOMAC (The Western Ontario and McMaster Universities Osteoarthritis Index) which
includes five questions about pain, two about stiffness and seventeen on degree of disability of activities performed every day11.
Following this, the subjects underwent hip abductor and vastus medialis oblique muscle (VMO) strengthening exercises namely clam shell, lateral leg slides, abduction lifts, terminal knee extension, single leg lifts, leg extension respectively for a total of 3 sets consisting 12 repetitions each .The exercises were given for 4 days in a week for total of 12 weeks. Subjects were advised to continue the medications as prescribed by their physician. After 12 weeks post exercise, they were subjected to Post Vas, WOMAC and findings were documented.
RESULT
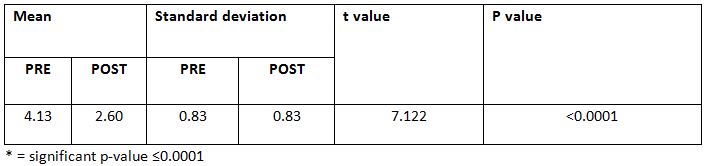
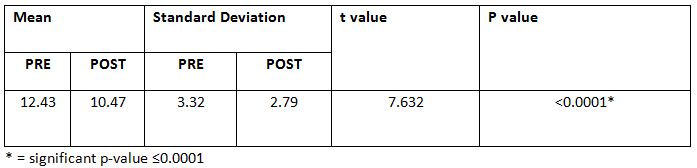
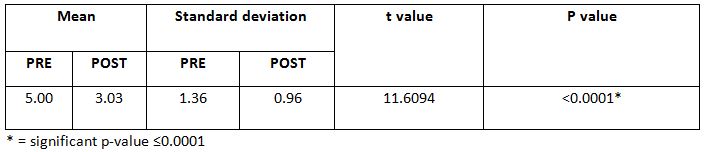
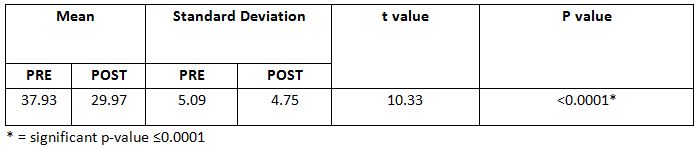
This study showed a substantial improvement of pain, stiffness and physical function in subjects who underwent VMO and hip abductor strengthening program. P-value on VAS and WOMAC scale was less than 0.0001 which was found significant.
DISCUSSION
This study was aimed to find the impact of hip abductor & VMO muscle strengthening in subjects with grade 1 osteoarthritis knee. Pain and Physical function was measured using VAS and WOMAC. The outcome of the study was markedly improved, on the WOMAC score after twelve weeks intervention program for the hip abductor and VMO in 30 participants.
In addition to the reduced dynamic loading at the knee, each subject experienced a marked decrease in knee pain during the study. VMO Strengthening served to reduce pain in subjects. The hip abductor plays an important role as pelvic and trunk stabilizer in locomotion 10.
The subjects gave a feedback on reduced gait deviations and improved stability during walking which is well evident from findings of Yujiexie, chi zhanget.al, (2018) who reported that the position of body center is depends on the strength of hip abductor weakness which
can alter in the contra lateral movement of the pelvis or lateral leaning of the trunk over the weight bearing lower extremity 11.
Knee adduction moment, associated with hip adduction has proved effect on reduce the disease severity on OA Knee. Hip abductor appears to have certain impact on knee joint load, which may also play a potential role in the symptoms, progression of disease & studies have pointed that hip abductor strengthening exercises may be helpful to improve the physical function & alleviate pain in OA knee12.
A study on lower limb muscle strengthening also have reported effect on reduce pain and potential ability at knee joint which is inexpensive treatment for OA. The findings are evident for the effects of hip abductor and VMO strengthening on relieving pain and improving physical function in knee OA subjects. Hip abductor strengthening routine can be included in grade-1 stage of knee OA as it can reduce the progression of the disease and improve quality of life.
Ethical Clearance: Ethical clearance has obtained from Faculty of Physiotherapy, DR.MGR. Educational and Research Institute, Chennai to conduct this study with reference number: A–026(A)/ PHSIO/IRB/2018-19dated 07/01/2019.
Conflict of interest: The author reported no conflict of interest to do this study
Funding: The researchers had self financial support to conduct this research.
Limitation: A small sample size, less study duration. Effect of medications was not taken into consideration.
Recommendations of the study: More outcome measure can be used. Several types of exercises can be compared for future studies. This study can be compared with other grades of KOA.
CONCLUSION
We can conclude that hip abductor and VMO strengthening is effective in reducing pain and improving physical function in subjects with grade- 1 KOA. Hence it can be included during the initial phase of rehabilitation of KOA.
REFERENCE
1. Hinman RS, Hunt MA, Creaby MW, Wrigley TV, Mc Manus FJ BK. (2010). Hip muscle weakness in individuals with medial knee osteoarthritis. Arthritis care Res. 62(8): 1190.
2. Michael JW, Schlüter-Brust KU EP. (2010). The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch Arzteblatt Int. 107(9): 152.
3. Gorial F I, Sabah S A, Kadhim M B J N. (2018). Functional Status in Knee Osteoarthritis and its Relation to Demographic and Clinical Features. Mediterr J Rheumatol. ; 29 (4): 207.
4. Zhang W, Doherty M, Peat G, Bierma-Zeinstra MA, Arden NK, Bresnihan B, (1962). Herrero-Beaumont G, Kirschner S, Leeb BF, Lohmander LS MB. Eular evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann Rheum Dis. 69(3): 483.
5. Sled E A, Khoja L, Deluzio K J, Olney S J C E. (2010). Effect of a home program of hip abductor exercises on knee joint loading, strength, function, and pain in people with knee osteoarthritis: a clinical trial. Phys Ther. 1 ; 90(6) :895-904.
7. Rutherford DJ H-KC. (2009). Explaining the hip adduction moment variability during gait: Implications for hip abductor strengthening. Clin Biomech. 1; 24(3): 267-73.
8. Harikesavan K, Chakravarty R D, Maiya A G, Hegde S P S S. (2017). Hip abductor strengthening improves physical function following total knee replacement: one-year follow-up of a randomized pilot study. Open Rheumatol Journal. 11:30.
9. Kellgren J H L J. (1957). Radiological assessment of osteo-arthrosis. Ann Rheum Dis.; 16(4): 494.
10. Yang KA, Raijmakers N J, Verbout AJ, Dhert WJ SD. (2007). Validation of the short-form WOMAC function scale for the evaluation of osteoarthritis of the knee. J bone Jt surgery Br Vol. 89(1): 50-6.
11. Xie Y, Zhang C, Jiang W, Huang J, Xu L, Pang G, Tang H, Chen R, Yu J, Guo S X F. (2018). Quadriceps combined with hip abductor strengthening versus quadriceps strengthening in treating knee osteoarthritis: a study protocol for a randomized controlled trial. BMC Musculoskelet Disord. 19(1): 1-7.
12. Lim BW, Hinman RS, Wrigley TV, Sharma L BK. (2008). Does knee malalignment mediate the effects of quadriceps strengthening on knee adduction moment, pain, and function in medial knee osteoarthritis? A randomized controlled trial. Off J Am Coll Rheumatol Care Res. 59(7): 943.
| Citation: Ishwarya vardhini. C, Nelshiya Anni Ruby Aishwariya. H. P (2021). Efficacy of Vastus Medialis Oblique Muscle and Hip Abductor Strengthening on Pain and Functional Ability in Patients with Knee Osteoarthritis, ijmaes; 7 (1); 969-974. |
Leave a Reply